- The Summary of Clinical Efficacy of in situ Skin Regenerative Restoration Technology (MEBT/MEBO) in the Treatment of Deep Ⅱ degree Burn Injures

-
目录
- 徐荣祥谈美国重复中国人体再生复原科学试验
- Dialogue with Xu Rongxiang about US Repeating Chinese Trial of Human Body Regenerative Restoration Science
- 人体多能干细胞体外定向分化形成肠组织
- 破解人体生命延续之谜(二)——线粒体主导日常生命
- Decoding the Mystery of Human Life Regenerative Extension (2)——Mitochondria dominate daily life
- 马克思主义与生命科学(Marxism and Life Science)
- 微小RNA表达模式的整体图谱区分干细胞类别
- 皮肤原位再生复原技术对深Ⅱ度烧伤治疗的临床疗效总结
- 长期低剂量服用阿司匹林可降低癌症死亡率
- The Summary of Clinical Efficacy of in situ Skin Regenerative Restoration Technology (MEBT/MEBO) in the Treatment of Deep Ⅱ degree Burn Injures
- 3682例小儿烧伤住院患者病因特征分析(Feature analysis of the causes of 3682 inpatients with pediatric burns)
- 湿润暴露疗法在黄磷烧伤治疗中的应用(Application of Moist Exposed Burn Therapy in the treatment of )
- 创疡贴在烧伤残留创面中的应用
- MEBO在外科手术切口感染的治疗
- 无需标记实时观察活组织中分子运动
- MEBO治疗大面积感染创面临床观察
- 老鼠实验表明修复端粒可以逆转衰老
- Does Moist Exposed Burn Ointment (MEBO)Promote Healing of Chronic Pressure Ulcers?——A Multicenteric Randomized Clinical Study
- 发现能显著减缓生物钟的化合物
- MEBO能促进慢性压力性溃疡的愈合吗?——一个前瞻性、多中心、随机的临床研究
- 耐力锻炼使心肌细胞增殖的机理
- 再生疗法治疗泛发性皮肤与皮下组织缺损的临床研究
- 发现新的抗癌免疫细胞
- 湿润烧伤膏治疗糖尿病足的临床体会
- 分子“开关”影响衰老和代谢疾病
- 游离植皮结合负压封闭引流技术治疗糖尿病足溃疡创面
- 美宝疤痕软膏防治瘢痕的临床研究
- 《中国烧伤创疡杂志》稿约
Authors place of work:The Chinese Burn Association of the Integrity of Traditional and Western Medicine, Beijing 100020, China(XIAO Mo,WANG Hong-sheng, CHEN Yong-chong);Department of Burns and Plastic Surgery, Nanshi Hospital Affiliated with Henan University, Nanyang, Henan 473065, China(ZHAO Jun-xiang);Aviation Industry Xiangfan Hospital, Xiangfan Hubei 443065, China(LI Jun,WANG Shi-you)
【Abstract】Objective Discuss and verify the clinical mechanism of in situ skin regenerative restoration technology in the treatment of deep Ⅱ burns, summarize the therapeutic effect of “somatic cells transform into stem cells and then regenerate skin tissue organ in situ”. Methods Describe the histological observation and signs of physical examination in the view of in situ skin regenerative restoration technology for the treatment of deep Ⅱ burns, analyze and summarize the histological changes and clinical manifestations of wounds in different stages as well as systemic treatment after standard treatment. Results Standard utilization of in situ skin regenerative restoration technology has evident therapeutic effect of in situ regeneration and restoration for both topical wounds of deep Ⅱ burns and systemic organs. Conclusion In situ skin regenerative restoration technology provides brand new therapy for patients with deep Ⅱ burns. The clinical outcomes indicate this therapy has significant therapeutic effect, strong practicability and advancement.
【Key words】Deep Ⅱ burns; In situ skin regenerative restoration technology; Potential regenerative cells; Histocyte; Stem cells; Skin organ; Clinical therapy
Deep Ⅱ degree burn injuries belong to the deep burn. It is the dermal burn injury according to the histological classification with the individualized pathological changes and clinical management. And the choice of therapeutic ways and the definition of clinical therapeutic effects are still controversial. Either the application of traditional ways (dryness of wound and escharectomy) or the application of in situ skin regeneration restoration technology is different in the terms of pain extents during the therapeutic process and the prognosis. In this article, in accordance with the authors’ clinical experience, the mechanism of the recoverability of the stagnation band (lies between the necrotic layer and the healthy layer) is analyzed from the features of deep Ⅱ degree burn histopathological changes, on the theoretical basis of ‘The transformation of PRCS into stem cells that in situ regenerate into skin tissue and organ; the foundational principles and applicant key-points of in situ skin regeneration restoration technology in the treatment of deep Ⅱ degree burn injuries are introduced; The scientificity and the clinical practical effects of the application of in situ skin regeneration restoration technology in the treatment of deep Ⅱ degree burn injuries without scar formation are verified through the histological changes at each stages of in situ regeneration restoration on wound bed with deep Ⅱ degree burn injuries and the standard clinical therapeutic progress and methods of in situ skin regeneration restoration technology.
1. The histopathological features of deep Ⅱ degree burn wound
The classification of in situ regeneration restoration technology to depth of burn wound is in line with anatomic structures—Burn Three Degree and Six Classifications that includes type of epidermal injuries, type of dermal injuries and type of full-thick dermal injuries. Deep Ⅱ degree burn injury is the type of dermal injury. According to is clinical manifestations, it can be divided into deep Ⅱ degree superficial type and deep Ⅱ degree deep type. Prof. Xu Rongxiang pointed out in the foundational studies of histopathological changes on burn skin that due to the temperature gradient (with high temperature in the necrotic layer and low temperature in the deeper layer), the increased capillaries permeability of affected area, the concentrated cellular contents of blood stream that leads to the slow rate, even stasis of blood stream, the red blood cells in capillaries are congested. With the persistent negative effects from temperature, the stasis of micro-circulation will occur quickly, then causing the occurrence of the pathological change—stasis zone[1]. Testified by clinical practice, the physiological moisture environment ensures the realization of the recoverability of stagnation band on wound bed. Jackson also believed that the position of stagnation band is different with the different burn depth. The stagnation band lying in deep dermal layer can be classified as deep Ⅱ degree burn injuries. De Camara observed that there were progressive damage around the stagnation band of cavia porcellus with deep Ⅱ degree burn injuries and the peak is about 8 hours after burn. And for 24 hours after burn, the stagnation band is self-limited. Both of the academic points have directive meaning for the feasibility and the applicant time limit in the early application of in situ skin regeneration restoration technology.
We concluded from the clinical practice, the affected skin tissue with deep Ⅱ degree burn injuries during the early stage is in shock status. The key intervention is to awake the PRCS (Potential Regenerative Cells) and positively rescue the stagnation band of the wound. PRCS are the foundation of in situ regeneration on wound bed and the rescue of stagnation band is the condition for in situ regeneration on wound bed. The pathological changes of stagnation band has close relationship with the changes of burn depth: the implementation of the effective interventions including the improvement of congested micro-circulation of stagnation band can effectively avoid the development of burn wound from deep Ⅱ degree to Ⅲ degree. The dryness and dehydration of burn wound is a reason for the aggravation of the blood stream congestion. The in situ skin regeneration restoration technology that can maintain the physiological moisture environment on wound bed is a kind of key and effective intervention to restore the congestion of blood stream on the stagnation band and promote the in situ regeneration restoration on wound bed.
2. The cytological foundation of in situ regeneration restoration on the wound bed with deep Ⅱ degree burn
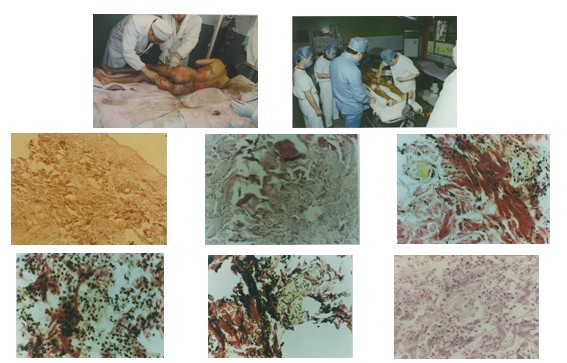
The dermal layer of the skin has been injured in the deep Ⅱ degree burn injuries, but as the existence of PRCS in the deep layer of the skin[2], after the application of MEBO Wound Ointment at the early stage of treatment, the wound then enters into the initiating stage of stem cells (12-24 hours after burn). By the action of the degeneration of necrotic tissue and the releasing of ‘death factor’, potential regeneration cells (PRCS) in the deep layer of the wound bed are awakened and begin to proliferate and differentiate that is the process of the transformation of somatic cells into stem cells. Meanwhile, from 24 hours to one week after injury, the cultivating stage of stem cells is stepped into(Fig. 1), the somatic cells in the model of embryonic development were proliferated and transformed into the regenerative procedures of skin tissue and cell(Fig. 2). In the process of continual standard application of MEBT/MEBO, the wound bed will finish the in situ regeneration with two weeks. The assemble of stem cells are formed in the model of embryonic development regeneration with the growth of multi-functional stem cells that means the procedure of regenerative skin tissue and organ is entered(Fig. 3). After three weeks’ standard application of MEBT/MEBO, the wound enters into the stage of in situ restoration that means the combination of multi-functional stem cells, including the growth of skin appendages, such as hair follicles, sweat glands and etc(Fig. 4). With the fusion of various stem cells and positioning on the normal skin structures(Fig. 5~6), the normal structure and function of skin tissues and organs recover by the protection of MEBO Wound Ointment.
Cast: Name: Li ××, female, 20 years old. Suffered from burn injuries by gasoline flame with TBSA 35% (Deep Ⅱ degree takes up to 15%, superficial Ⅲ degree 20%), for ten hours after burn, the client was admitted. Then, MEBT/MEBO was immediately administered during the entire treatment. 30 days later, the wound was in situ regenerated and restored.
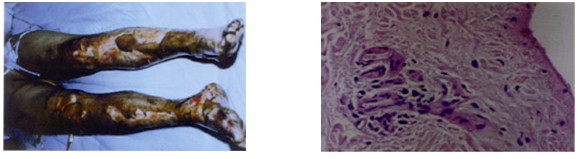
Fig.
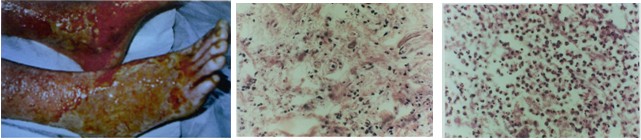
Fig.

Fig.
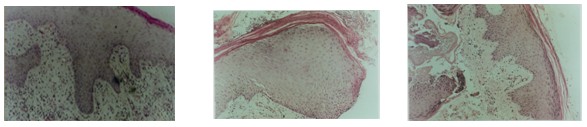
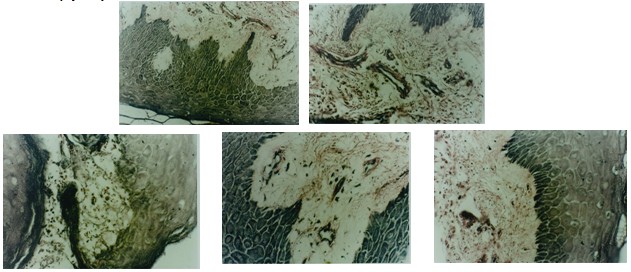
Fig.
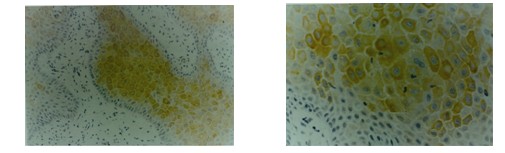
Fig. 6with the keratin staining by immunohistochemistry: a.the active growth of skin cells by the way of in situ regeneration; b.the active growth of the cells in the stratum granulasum.
3. The histological observation and clinical process of in situ regeneration on deep Ⅱ degree burn wound
3.1. The histological observation of in situ regeneration on deep Ⅱ degree burn wound
10 days after the treatment by MEBO/MEBO, the tendency of epidermal regeneration and restoration appears fine with the preferable regeneration of spinose cells. And the cytosplasm of the surrounding cells is prominent and connected by desmosome. Observed under the electron microscope with 3000-20000 multiple, the interval space among the adjacent cellular membranes is 20-30NM with the filling of filiform substances that are interweaved into a compacting line at the center axis. The compacting substances on the surface of two adjacent membranes contribute the adhering plate. Some thin filament with tension is attached to the plate that presents fundiform retracing matrix.Under the observation by electron microscope, the stratum basale could be seen. The cells laid in the stratum basale are the strongest power in splitting and proliferation; the lateral and superficial sides of basilar cell are connected by desmosome, and the inferior side is connected with basement membrane by semi-desmosome (Fig. 7).
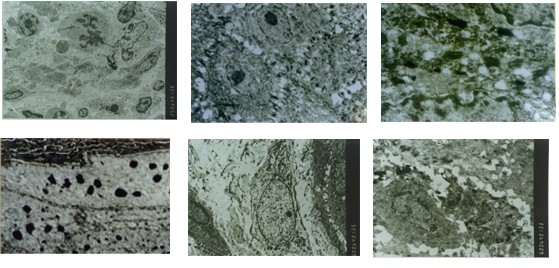
Fig. 7The observation by electron microscope to the super micro-structure of skin tissues treated by MEBT/MEBO: a.the phenomenon of slitting of nucleus appeared four days after the application of MEBT/MEBO on deep Ⅱ degree burn; b.cten days later, spinous cells (regenerated) connected with the surrounding cells by desmosome. Observed under the electron microscope with 3000-20000 multiple, the interval space among the adjacent cellular membranes is 20-30NM with the filling of filiform substances that are interweaved into a compacting line at the center axis. The compacting substances on the surface of two adjacent membranes contribute the adhering plate. Some thin filament with tension is attached to the plate that presents fundiform retracing matrix; d~f.under the observation by electron microscope, the stratum basale could be seen. The cells laid in the stratum basale are the strongest power in splitting and proliferation; the lateral and superficial sides of basilar cell are connected by desmosome, and the inferior side is connected with basement membrane by semi-desmosome.
(1) Fibrocytes: The relationship between the in situ regeneration of skin tissue and fibrocyte is rather intimate. The number of fibrocytes in the regenerated dermal tissue is 4 times larger than epithelial cells. MEBO Wound Ointment can promote the maturation of fibrocytes and the production of collagenous fiber, elastic fiber, reticular fiber and matrix. The process of promoting the maturation of fibroctyes is the process that MEBO Wound Ointment promotes the in situ regeneration restoration of burned skin tissues with reduction or prevention of scar formation(Fig. 8).
(2) The observation of various cells, includes macrophage(Fig. 9), plasma cells, mononuclear cells, white blood cells, mast cells and etc.
①Macrophage: it is differentiated from mononucleocyte after passing through vessel. After it enters into the connective tissue, its volume will be enlarged with increased lysosomes and the power of swallowing capability. It either has the defense function, involving in the modulation of immune response or excretes multiple bioactive substances (including interleukin I, lymphocyte activation factors). Ultimately, the targeted cells (bacterias, necrotic cells and etc) are killed.
The results after the observation by electron microscope: 15 days’ treatment after MEBO Wound Ointment, the mononucleocyte and macrophage are comparatively active that are implicated in the improvement of immunity.
②Plasma cell: plasma cell is transformed from B lymph cell under the repetitive stimulation by antigen (inflammatory mediator and etc). It can produce immune globulins or antibodies.The results after the observation by electorn microscope: 4 days after the application MEBO Wound Ointment on burn wound, it shows the biochemical process that B lymph cell is transformed into plasma cell.
③Mast cell: it is hardly observed on the patients in this group, except for one with lowered socioeconomic status.
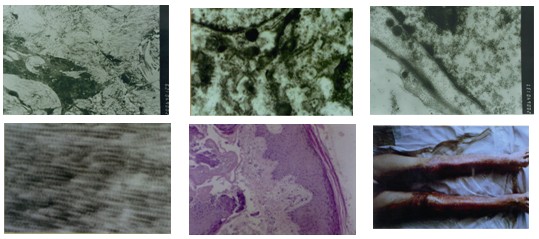
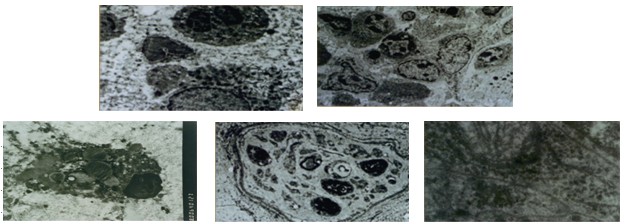
Fig. 9Various cells, including macrophage, plasma cells, mononuclear cells, white blood cells, mast cells and etc. a.macrophage and plasma cells are the cells that are transferred from B lymphocytes due to the repeated stimulation by antigens (inflammatory mediator and etc) with the function to secret immune globulin or antibodies; b.4 days after the application of MEBT/MEBO on burn wound, B lymphocyte in the wound bed begans to transverse to plasma cell. Mononulear cells c.mast cells d.the mast cells were found in the wound bed with bad overall conditions; e.neutral cells (neutral fibers) were in situ regenerated, and the typical neutral fibers were found 15 days after the injuries.
The wound is applied MEBO Wound Ointment at the early stage, the initiative stage of stem cell is stepped (12-24 hours after burns), by the action of the degeneration of necrotic tissue with the releasing of ‘death factor’ and MEBO Wound Ointment, PRCS locating in the deep layer of wound is awakened and begin to proliferate and differentiate that somatic cells start to be transformed into stem cells.
3.2. The clinical process of the in situ regeneration on the deep Ⅱ degree burn woundBy the way of clinical observation in combination with the studies of pathological histology, the laws of the clinical process of the in situ regeneration on the deep Ⅱ degree burn wound as followed are induced:
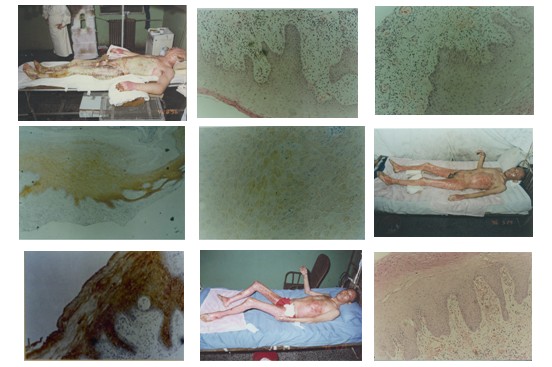
Case: Name: Ma ××, male, 50 years old. He suffered from scald by steam with TBSA up to 77% (deep Ⅱ degree takes up to 50%, superficial Ⅲ degree 27%). The client was admitted 7 hours after injury. Then MEBT/MEBO was given during the entire process of treatment. The deep Ⅱ degree wound was in situ regenerated and restored after 30 days’ treatment. For 45 days’ treatment, the wound classified with superficial Ⅲ degree was in situ regenerated and restored without skin-grafting. For another 3 months’ physical exercise, the client’s normal life and work were fully returned without dysfunction left (Fig. 10~11).
4. The basic principles and application key-points of in situ Skin Regenerative Restoration Techniques in treating deep Ⅱ degree burns
The key-points required during the clinical application of In Situ Skin Regenerative Restoration Techniques in treating deep Ⅱ degree burns are as follow: based on the basic theory of in situ regenerative restoration of skin tissues and organs with Human Body Regenerative Restoration Science, and the principle of guiding clinical practices with the physiological process of‘the transformation of somatic cells into stem cells to regenerate skin tissues and organs in situ’[4], protect injured tissues, and exclude any unfavorable factors for tissue regeneration, finally realizing the in situ regenerative restoration of the diseased and injured tissues and organs[5~6].
Details can be summarized as follows: (1) Early administration of MEBO Wound Ointment: smear MEBO within 12~24 hours post injury onto the wound beds (MEBO plays as wound cleaning agent), so as to initiate and activate the PRCS in the wound beds to transform them into stem cells; administration of MEBO Wound Ointment during the entire course of therapy: promise the persistent and timely supplement of regenerative nutrients—MEBO on wound beds to complete the process of in situ skin regenerative restoration; standardized procedures: correctly use the In situ Skin Regenerative Restoration Techniques—MEBT which makes the regenerative restoration of skin tissues and organs on wound beds in accordance with physiological process.
4.1.Basic principles
The general treating principle of deep partial thickness burns (deep Ⅱ degree burns) including superficial and deep types is to create the environment for physiological wound regeneration on the premises of ensuring the successful transformation of PRCS into stem cells and in-situ regeneration of skin tissues and organs, with the following basic principles:
4.2.Purpose of treatment
4.3.Key-points of the application of in situ skin regenerative restoration technique on deep Ⅱ degree burns at all stages
General key-points for deep Ⅱ degree burns treatment: during the treatment, the MEBO Wound Ointment should be considered as culture medium to exert its cultivating effect of in situ skin regeneration, but not as medicine, for it is the nutritional agents going with the in situ regenerative restoration of wound which is different from the antagonistic effect of modern pharmacology; on the other hand, MEBO Wound Ointment need to be used as cleansing agent to protect the fresh or new wounds and get rid of foreign contaminations, which has been confirmed by amazing results in clinic. As a result, the earlier application of MEBO Wound Ointment is the key to the initiation of PRCS on the wound beds for regenerating new skin tissues.
From day 8 to day 14 post-injury, the key point is to maintain the physiologically moist environment with standard application of MEBT/MEBO on local wound. During this stage, adhere to principles as follow: maintenance of the patency of the wound drainage, timely administration of MEBO and dressing-change. In order to accelerate the liquefaction of necrotic tissues on deep Ⅱ and Ⅱ-Ⅲ mixed wounds, it is required to timely get rid of the liquefied substances, sloughing and blister wall from the wound while supplying sufficient MEBO ointment.
4.4.Clinical manifestations of wounds should be observed and managed throughout the course of treatment
From day 15 to day 21 post-injury, in the physiologically moist environment created by MEBT/MEBO, multi-functional stem cells have been formed and the appendages of skin start generating. Various stem cells fuse with each other and locate their belonging skin tissue positions, and then develop to the normal physiological structure. During this stage, the necrotic tissues on the wounds should be completely discharged with the coming of the newborn granulation tissue. The key-point during this stage is the protection of wound bed. The interval of dressing-change can be lengthened to once per 6 to 8 hours. Make sure there is no accumulation of residues on the wound bed during the dressing-change in order to heal the wound by the way of in situ regenerative restoration.
4.5.Continue treatment of wound at rehabilitation stage is required to make sure the optimal restoration result
From day 22 to day 28 post-injury, the physiological and anatomic structure of skin tissues and organs has formed with various skin functions restoration gradually. It is required administering continuous rehabilitative interventions to the regenerated or newborn skin. The one is the scar-prevention therapy. The other is the treatment on the hemorrhagic vesicles and blisters appearing on the skin surface after the movement of affected skin. For the burns that the depth reaches to deep Ⅱ degree and more, the scar-prevention therapy after wound healing should routinely be given. The detailed procedures are continuously the application of MEBO ointment for 2 weeks after wound healing, then start administering MEBO Scar Ointment three times per day and massage with palms after each administration for 15 minutes to promote the sufficient absorption of MEBO Scar Ointment so as to strengthen the anti-scar effect. For the skin with hemorrhagic vesicles and blisters formed after movement of affected areas, it can use the sterile injector to draw the in-side blood or fluid, and then smear a small amount of MEBO ointment onto the affected area 4 times per day. The affected areas will be healed rapidly. At this time, we should inform patient to have proper exercises and the necessity to avoid the long-term dependent position of lower extremities.
From day 29 to day 90 post-injury, with the assistance of systemic supplement of regenerative substances and dietary adjustment, the overall restoration of the body finishes via the systemic neuromodulation on the regenerated skin structures and functions.
5.The wound appearance and standard application of MEBT/MEBO of deep Ⅱ degree burns
The deep Ⅱ degree burns can achieve total regeneration and restoration with no scar formation and dysfunction left If the standard application of MEBT/MEBO is performed. But if the wound were treated incorrectly, the curing periods might be lengthened that suffer the patient more and increase the burden of economy. Sometimes, even cause the scar formation and cosmetic problems with dysfunction left so as to lower the work and life quality. According to the different depth of injury, it can be classified into two types: partial thickness superficial type and deep type[7-8].
5.1.The wound treatment of partial thickness burns superficial type (deep Ⅱ degree superficial type)
This type of burns reaches down to the reticular layer of dermis with the damage of papillary layer. Generally, there are big or small blisters formed with thick blister wall. The blister wall is insusceptible to separate after drainage of the in-side fluid. Three to four days after the treatment with MEBO ointment, If the wound surface appears red and white, or the whitish wound with red spots, it is considered as injury on the superficial dermis. In another word, the papillary layer of dermis has already injured and died with the congestive microcirculation at the reticular layer. With the action of MEBO ointment, some part of the microcirculation can be reopened. But it is necessary to avoid the wound exposure in the air as a result of the insufficiency of MEBO ointment protection during the treatment. The wound bed should be timely supplied with MEBO ointment to maintain the wound in the physiologically moist environment created by isolation membrane, assuring in situ regeneration of stem cells (Fig. 12).
5.2.The wound treatment of partial thickness burn deep type (deep Ⅱ degree burn deep type)The burn causes the injury down to the reticular layer of dermis, but parts of the deep structure in the deep layer of dermis and subcutaneous that locates the skin appendages still remain reactive. From the histological prospective, the microcirculation stagnation has formed in the reticular layer. During the inspection, there is no or dispersed small blisters on the wound surface, yellow or waxy eschar forming (the color of eschar appears tan if the burn is cause by flame). Through the eschar, it could be observed the tiny disperse red points or dark brown spots that indicate the signs of congestion or partial obstruction in the capillary plexus around remnant skin appendages. Since the most nerve endings have injured or died, the pain is not apparent. The temperature on the wound surface is slightly lower than normal with dull pain feeling during palpation. The typical characteristic of this kind of burn is the formation of ‘band of inflammatory infiltration’ between the superficial necrotic layer and the deep surviving tissues. When administering the traditional dry therapy, this kind of ‘band of inflammatory infiltration’ becomes the foundation of the wound secondary infection. To promote the eschar formation with the dry hot wind will make this band of inflammatory infiltration necrotic and deepen the wound. Whereas, during the application of MEBT/MEBO, the wound protected by MEBO at the early stage (within 12 hours after burn) can efficiently reduce the process of inflammation; at the same time, the permeable effect of MEBO makes the capillaries in the stagnated tissues unobstructed, then the physiological functions are restored. The purpose of the early application of MEBO is to revitalize the agonal tissues in stasis zone by the virtue of effective substances of MEBO prior to the incomplete formation of ‘band of inflammatory infiltration and the beginning of the rejection (Fig. 13)[10].

The liquefied stuff totally is discharged about at the 13th to 15th day after MEBO treatment. After that, the repairing stage of the wound begins. The exposed wound basal appears red with the white spots and net-like matter coating on the wound basal formed by the residual skin appendages (sweat glands and etc) in the physiologically moisture environment. At this time, pay attention to maintain the consistent supplement of MEBO Wound Ointment and avoid the dryness on the wound beds. As the number of collagen cells in the epithelial tissue would rise to the top at the 20th day after administration of MEBO according to its life circle. If the wound were administered the bandage with pressure to promote the healing, the collagenous fiber would continue proliferating and forming into the scar texture. But the collagen cells exposed in the physiologically moisture environment created by MEBO Wound Ointment can be completely matured. This kind of wound can be prevented from the scar formation after healing.
To be emphasized, during each dressing change, it is required to observe the sign of infection on deep wound, especially on the pressed or therapeutic puncture site. If there is deep abscess observed, timely perform incision and drainage to remove infection risk.The wound appears red during the early stage of wound healing with level higher than the surrounding skin.
At this time, the MEBO Wound Ointment should be continuously applied onto the wound to maintain the wound moisture. As the regenerative healing, at this time focuses on the regeneration of dermis, the epidermal layer still has not completely regenerated and repaired. Yet, the wound surface is protected by MEBO Wound Ointment replacing the epidermal function. After about 15 days, the epidermal cells can be fully regenerated and repaired. About 30 later, the cuticular layer can be basically formed. It should be emphasized that the functional exercises should be enhanced on the affected extremities during the treatment of MEBT/MEBO. The activity and exercises can promote the local blood circulation and the nutritional supplement of epithelial regeneration which is greatly beneficial for the healing of the wound and the foundation of the rare incidence of dysfunction after the treatment with the standard in situ Skin Regenerative Restoration Technique for the extensive burns.
6.The standard systemic therapy in the application of the in situ Skin Regenerative Restoration Technique on deep Ⅱ degree burns
Burns is an injure on body system, and deep Ⅱ degree burns is not only a damage to the skin tissues and organs, especially for medium or extensive burns with TBSA>30%. Hence, when in situ Skin Regenerative Restoration Techniques (also called as Burn Regenerative Therapy) is used in the management of burns, the first key point is to offer the various in situ regenerative conditions for skin; second, the protopathy and complications need to be intervened at the same time. These are the principles that must be made clear. The general principle of treatment is to apply standard in-situ skin regenerative restoration technique in systemic treatment of burns, based on which infection prevention and control as well as systemic organ function protection is the indispensible treating focus.
The principle of ‘bacterial and toxin should be treated concurrently’ proposed by Xu Rongxiang in the systemic treatment of burns with sensible application of antibiotics[11]. Three major factors that determine the infectious degree of burns are the number of bacterial, the bacterial virulence and the patient’s immunity. The application of antibiotics is necessary in burn treatment, but It is required to use it timely and properly. Under such principle and therapy, Dr. Zhang Xiangqing has achieved ideal clinical results in treating extensive deep burns[12]. For deep Ⅱ degree burn with TBSA within 15%, close observation is required on general condition including body temperature, blood gram, without the need of antibiotics if not necessary. For burns with TBSA from 15%-30%, selected antibiotics should be chosen with the consideration of the toxic effect especially on renal function. The experience on antibiotic application is summarized as follow: ①empirical application: In order to prevent the occurrence of the invasive systemic sepsis and enterogenic infection at the early stage, the broad-spectrum, high-efficacy and low-toxicity antibiotics should be administer on admission; ②therapeutic application: Once the patient has the symptoms and signs of sepsis in clinic, do not wait the result of blood culture and administer the broad-spectrum, high-efficacy and low-toxicity antibiotics to control the infection.
Empirical length of antibiotic application: no more than 7 days. Then check CBC (complete blood count) daily to observe if there has toxic granulation in neutrophilic granulocyte. If it had, the more sensitive antibiotics should be chosen on the basis of the result of blood culture and wound bacterial culture. If it had not, the antibiotics should be stopped as soon as possible and continue the observation of patient’s overall status. Bear in mind hyperthermia is not the indicator of antibiotic applciation; therapeutic length of antibiotic application: Generally speaking, the board-spectrum antibiotics should be used for 3 – 5 days with timely administration and decisive discontinuance.
The anti-infection therapy indicators: ①Temperature higher than
The protection of vital organs’ function is the important issue in treating extensive deep Ⅱ degreed burns[13-14]. Systemic organs may be all damaged by shock or other complications after burns[15]. In accordance with the principles of Human Body Regenerative Restoration Science, whether the impairment is local or involves the overall tissues and organs, the physiologically moisture environment is supposed to be created to achieve the readjustment and repairing by regenerative restoration of overall organs’ dysfunction. In the treatment of medium and extensive deep Ⅱ degree burns, systemic organs’ protection is also emphasized. The basic principles include strengthening cardiac function, protecting renal function, and using urinary volume (UV) as the criterion for the maintenance of effective blood volume, and the general principle is to apply standard in-situ skin regenerative restoration technique in systemic treatment of burns[16].
References
[1]Xu Rongxiang(2008). The Complete Book of Burn Treatment [M]. Chinese Science and Technology Press, 24~28.
[2]Xu Rongxiang (2000). The trial study of the anti-bacterial effect of MEBT/MEBO [M]. Blue Book of MEBT/MEBO. Beijing. Chinese Medical Science and Technology Press. 94.
[3]Xu Rongxiang (2000) The study report of MEBT/MEBO to the epithelial stem cells [M]. Blue Book of MEBT/MEBO. Beijing. Chinese Medical Science and Technology Press. 64.
[4]Xu Rongxiang (2007). The declaration for the safeguard of life science and national dignity (White Book).
[5]Li Tianyu, Zhao Junxiang (2005). Experience in the rescue of large area burn patients in group. The Chinese Journal for Burns, Wounds and Surface Ulcers. 17(3): 196~198.
[6]Xiao Mo (1999). Histological Observation On The Effect Of MEBT/MEBO On promoting The Rrgeneration And Repair Of Deep Burn Wounds. The Chinese Journal for Burns, Wounds and Surface Ulcers. 11(3):1~3.
[7]Zhao Junxiang (2002). Report on Clinical Application of Burn Skin Regeneration Medical Technique. The Chinese Journal for Burns, Wounds and Surface Ulcers 14(3):192~193.
[8]Li Jun(2004). A comparative study of the efficacy of MEBT and surgical treatment for treating deep second degree burn wounds in dorsum of hand. The Chinese Journal for Burns, Wounds and Surface Ulcres. 16(4):271~273.
[9]Wang Hongsheng (2000) Comparative Analysis of the Efficacy of Dry and Moist Therapy in Treating
[10]Wang Hongsheng (2000). Factors Influencing the Efficacy of MEBO in Treating Facial Burn (A Report of 830 Cases). The Chinese Journal for Burns, Wounds and Surface Ulcers. 12(4):25~27.
[11]Zhang Xiangqing (2005). Clinical research on MEBO for treating burns with an area over 50% TBSA Report Ⅰ. The Chinese Journal for Burns, Wounds and Surface Ulcers. 17(3):169~177.
[12]Xu Rongxiang (2000). The trial study of the anti-bacterial effect of MEBT/MEBO [M]. Blue Book of MEBT/MEBO. Beijing. Chinese Medical Science and Technology Press. 94.
[13]Xu Rongxiang (2006). The health care of GI regeneration restoration [M]. Taihai Press.
[14]Xiao Mo and etc (2006). The present status of the application and research on gastrointestinal mucosa organ in situ regenerative restoration technique. [J]. The Chinese Journal for Burns, Wounds and Surface Ulcers. 18(3):165~170.
[15]Xiao Mo (2007). Recommended protocol of treating stress ulcers with regenerative restoration technique in situ. The Chinese Journal for Burns, Wounds and Surface Ulcers. 19(4):287~289.
[16]Xiao Mo (2010). Clinical Application of Skin Regenerative Restoration Therapy in Situ in Systemic Treatment of Burn Patient. The Chinese Journal for Burns, Wounds and Surface Ulcers. 22(4):25.