- Does Moist Exposed Burn Ointment (MEBO)Promote Healing of Chronic Pressure Ulcers?——A Multicenteric Randomized Clinical Study

-
目录
- 徐荣祥谈美国重复中国人体再生复原科学试验
- Dialogue with Xu Rongxiang about US Repeating Chinese Trial of Human Body Regenerative Restoration Science
- 人体多能干细胞体外定向分化形成肠组织
- 破解人体生命延续之谜(二)——线粒体主导日常生命
- Decoding the Mystery of Human Life Regenerative Extension (2)——Mitochondria dominate daily life
- 马克思主义与生命科学(Marxism and Life Science)
- 微小RNA表达模式的整体图谱区分干细胞类别
- 皮肤原位再生复原技术对深Ⅱ度烧伤治疗的临床疗效总结
- 长期低剂量服用阿司匹林可降低癌症死亡率
- The Summary of Clinical Efficacy of in situ Skin Regenerative Restoration Technology (MEBT/MEBO) in the Treatment of Deep Ⅱ degree Burn Injures
- 3682例小儿烧伤住院患者病因特征分析(Feature analysis of the causes of 3682 inpatients with pediatric burns)
- 湿润暴露疗法在黄磷烧伤治疗中的应用(Application of Moist Exposed Burn Therapy in the treatment of )
- 创疡贴在烧伤残留创面中的应用
- MEBO在外科手术切口感染的治疗
- 无需标记实时观察活组织中分子运动
- MEBO治疗大面积感染创面临床观察
- 老鼠实验表明修复端粒可以逆转衰老
- Does Moist Exposed Burn Ointment (MEBO)Promote Healing of Chronic Pressure Ulcers?——A Multicenteric Randomized Clinical Study
- 发现能显著减缓生物钟的化合物
- MEBO能促进慢性压力性溃疡的愈合吗?——一个前瞻性、多中心、随机的临床研究
- 耐力锻炼使心肌细胞增殖的机理
- 再生疗法治疗泛发性皮肤与皮下组织缺损的临床研究
- 发现新的抗癌免疫细胞
- 湿润烧伤膏治疗糖尿病足的临床体会
- 分子“开关”影响衰老和代谢疾病
- 游离植皮结合负压封闭引流技术治疗糖尿病足溃疡创面
- 美宝疤痕软膏防治瘢痕的临床研究
- 《中国烧伤创疡杂志》稿约
Mahmoud F. SakrCHEN Yong-chongAhmed K. Al-Batanouny
Authors place of work: Department of Surgery, Faculty of Medicine, University of Alexandria, Egypt And Department of Surgery, Ahmadi Hospital, Kuwait Oil company (KOC), Ahmadi, State of Kuwait(Mahmoud F. Sakr);100020China Beijing,Department of Burns, Wounds and Ulcers of China Science & Technology Center And Beijing MEBO Institution of Burns, Wounds and Ulcers(CHEN Yong-chong);Department of Surgery, Faculty of Medicine, University of Cairo, EgyptAnd Department of Surgery, Doha Clinic Hospital, Qatar(Ahmed K. Al-Batanouny);Department of Burn and Plastic of Hospital Sungai Buloh Ministry of Health Kuala Lumpur, Malaysia(Ibrahim Salina);100056China Beijing,Burn and Wound Center of Beijing XuanWu Chinese Traditional Hospital(ZHANG Yong);545002China Liuzhou,Department of Burn and Plastic of GuangXi LiuGang Hospital(LI Shi-bin, HUANG Gui-mei)
【Abstract】Objectives A multi-centers, randomized, controlled study to assess the efficacy and safety of MEBO (Julphar Gulf Pharmaceutical Industries, UAE, and SanTou MEBO Pharmaceutical CO., LTD., China) in healing of chronic pressure ulcers. Subjects and Methods Eighty seven patients with 182 chronic pressure ulcers treated at five hospitals from different areas in world, between January 2003 and January 2009, were randomized into 2 groups; those in group 1 (n=46) received MEBO while those in group 2 (n=41) received Fucidin (Leo Pharmaceutical, Denmark). Data collected prospectively included demographics, nutritional status, underlying predisposing disease and co-morbidities. Ulcer surface area (SA) and healing index (HI) were calculated and compared at two-week intervals for 12 weeks. Results Patients in both groups had similar demographic, clinical, biochemical features, and ulcer characteristics. There was a significant increase in HI and reduction in ulcer SA on weeks two and four respectively, that was maintained through 12 weeks in patients treated with MEBO. More than half of ulcers (56.5%) treated with MEBO had complete healing (HI = 1) by 12 weeks, as opposed to only 19.6% of those treated with Fucidin (P<0.001). Moreover, none of the patients receiving MEBO had a HI of <50% of their ulcers by 12 weeks as compared to 26.8% of those receiving Fucidin (P<0.001). No adverse effects or allergic reactions of topical ointment were encountered in either group. Conclusions In addition to its safety, MEBO significantly promotes the healing of chronic pressure ulcers with significant increase in HI of any given ulcer as early as two weeks following initiation of treatment, and complete healing of more than 50% of ulcers by 12 weeks.
【Key Words】MEBO; physiological moist environment; regenerative medicine; pressure ulcers; chronic wounds; healing index
【Article identifier】doi:10.3969/j.issn.1001-0726.2011.01.010
INTRODUCTION
Pressure ulcers, defined as any lesion caused by unrelieved pressure resulting in damage of underlying tissue, constitute a clinical challenge for both the clinician and the patient[1]. Healing is unpredictable, it often stalls due to such local factors as sepsis, edema, and prolonged pressure; and to systemic factors such as diabetes mellitus, smoking, anemia, poor nutrition, obesity, cancer, ischemia, uremia, and denervation. Chemotherapeutic agents, corticosteroids and tissue irradiation also lead to delayed wound healing[2~3].
There is, however, recent evidence in the literature that good hydration is the single most important external factor responsible for optimal wound healing[4~6]. Moist Exposed Wound Ointment (MEBO) (Julphar Gulf Pharmaceutical Industries, UAE., and SanTou MEBO Pharmaceutical CO., LTD., China) reduces evaporation from the wound surface, thereby offering a moist environment for wound healing[7]. It has no evident negative effect on the immune defense mechanisms[8], and has a similar action in-vivo to Silver Sulfadiazine in controlling burn wound sepsis and systemic infection with P. aeroginosa[9]. It has also been shown experimentally that MEBO exhibited a significantly superior wound healing potential on rabbit corneal epithelium as compared to saline, homologus serum, vitamin A and dexamethasone[10], as well as on rabbit skin burns treated with Vaseline[11]. Moreover, MEBO has been found to be extremely beneficial in the treatment of partial thickness facial burns[12], and split thickness skin graft donor sites[13], and for the healing of experimentally induced CO2 laser burns in animals[14].
The present randomized clinical study was therefore conducted to assess the efficacy and safety of MEBO as compared to topical antibiotic ointment (Fucidin, Leo Pharmaceuticals, Denmark) in the local wound care and healing of chronic pressure ulcers.
1.SUBJECTS AND METHODS
1.1.Study Population
The present study included 96 patients with 196 chronic pressure ulcers seen at five different hospitals between January 2003 and January and 2009. Nine patients with 14 ulcers were lost during the early follow-up and were thus excluded from the study. The remaining 87 patients with 182 ulcers constituted the study population of the present clinical trial.
All data was collected prospectively and included demographics, nutritional status, underlying predisposing disease and/or co-morbidities such as diabetes mellitus, peripheral vascular disease, renal insufficiency, malignancy, connective tissue disease, central nervous system, spinal cord or peripheral nerve injuries, endocrinopathy, and chronic osteomyelitis. Previous irradiation, and concomitant corticosteroids or chemotherapy administration were noted. Adverse reactions or hypersensitivity reactions to the topical agent, if any, were also recorded. There were 48 men and 39 women. Their ages ranged between 14 and 102 years with a mean of 69.5?9.4 years. Patients had their ulcers prior to study entry for a mean of 10.67 months (range 2~27 months).
1.2.Study Protocol
This prospective randomized study was conducted from Jan 2003 to Jan 2009 at five different hospitals after approval of the protocol by each Hospital Ethical Committee. After obtaining consent of the patients or their first-degree care-givers, patients of both sexes with chronic pressure ulcers failing to heal for more than six weeks were enrolled in the study. The pressure ulcer staging system adopted by the panel developing the pressure ulcer treatment guideline for the AHCPR in 1994[15] was utilized in this study. Patients were randomized, using the sealed envelop method. Those in group 1 (n=46) had a 96 ulcers and received MEBO, while those in group 2 (n=41) had 86 ulcers and received Fucidin.
Local wound management was accomplished by twice daily application of a thick layer of ointment (1~
Laboratory investigations for all patients included complete blood count, hematocrit, hemoglobin, liver function tests, blood urea and creatinine, serum electrolytes, and blood glucose levels.
1.3.Healing Index
Healing index (HI) was calculated by dividing the difference in ulcer size between “day
Healing Index (HI) = (ulcer size day 0 - ulcer size day x) / ulcer size day 0.The HI thus ranges between 0-1, where 0 means no healing (as compared to day 0), and 1 means complete healing, irrespective of ulcer size.
1.4.Statistical Analysis
Data were analyzed using the SPSS/PC version 12 computer software (Prentice-Hall, Chicago, IL). Continuous variables were expressed as mean values and standard error of the mean (X ? SE), and were compared using the students t test. Differences in ulcer surface area were compared using a non-parametric test (Menn-Whitney’s) due to wide range. The Chi-square test was used to compare proportions including those of healing ulcers at 12 weeks after initiation of treatment. Probability value of < 0.05 was considered to be statistically significant. A linear regression analysis was also performed calculating r2 values in order to evaluate the change in ulcer size and healing index that can be attributed to ointment application. Owing to the relatively small sample size, r2 values more than 0.4 were considered to indicate that the two parameters are in correlation with each other whereas values less than 0.4 indicated that other variables may have contributed to the observed changes in ulcer size.
2.RESULTS
Patients in both groups had similar demographic and clinical features regarding their age, gender, underlying predisposing factor for ulcer development, and associated medical conditions, in addition to their laboratory results (anemia and hypoalbuminemia). Cerebro-vascular accident (CVA) was the most common predisposing factor, and diabetes mellitus and hypertension were the most common co-morbidities, in both groups (Table I). Ulcer characteristics were also similar regarding their number, site, size, duration, depth and presence or absence of sepsis (Table II). In both groups, the number of ulcers per patient ranged between one and four, the trochanteric region was the most common ulcer site, and stage III ulcers were the most common at the time of initiation of treatment. No skin grafts or flaps were needed to close the wounds in the MEBO groups as opposed to 12 patients who required skin grafts in the Fucidin group. Four patients died in each group after 7~13 months of their enrollment in the study, which did not affect the data gathered regarding healing of their pressure ulcers.
Table I Clinical and Biochemical Features of Patients in Both Studied
GroupsClinical Features
Group 1 (MEBO), n=46
Group 2 (Fucidin), n=41
Age (Years):
● Mean±SD:
● Range:
67±8.5
14~95
73±9.2
25~102
Gender:
● Male:
● Female:
26 (56.5%)
20 (43.5%)
20 (48.8%)
21 (51.2%)
Predisposing Factor:
● Old CVA
● Paraplegia
● Cerebral Palsy
35 (76.1%)
7 (15.2%)
4 (8.7%)
29 (70.7%)
9 (22.0%)
3 (7.3%)
Co-morbidities:
● DM
● Hypertension
● DM + Hypertension
● Renal Failure
● Cardiac Disease (LVF)
● Neoplasia:
- Brain tumor
- Ovarian cancer
- HCC
19 (41.3%)
9 (19.3%)
6 (13.0%)
5 (10.8%)
5 (10.8%)
2 (4.8%)
1
1
0
19 (46.3%)
8 (19.5%)
5 (12.2%)
5 (12.2%)
3 (7.4%)
1 (2.4%)
0
0
1
Laboratory Results:
● Hemoglobin (g/dl)
● Albumin (g/dl)
10.3±1.1
31±4.3
10.3±1.1
31±4.3
Vital Status:
● Survival:
● Death:
42 (91.3%)
4 (8.7%)
37 (90.2%)
4 (9.8%)
CVA: Cerebro-vascular accident, DM: Diabetes mellitus, LVF: Left ventricular failure, HCC: Hepatocellular carcinoma. All differences were not statistically significant (P>0.05).
Table II Ulcer Characteristics of Patients in Both Studied Groups
Ulcer Characteristics
Group 1 Ulcers (MEBO)(n=96)
Group 2 Ulcers (Fucidin) (n=86)
No. of ulcers / patient
● One ulcer:
● Two ulcers:
● Three ulcers:
● Four ulcers:
No. of Patients
16
14
12
4
No. of Patients
14
12
12
3
Duration prior to entry (months):
● Mean±SD:
● Range:
8.86±6.9
2~26
11.57±7.5
72~24
Ulcer Site:
● Trochanteric:
- Right:
- Left:
● Sacral:
● Heel:
- Right:
- Left:
● Shoulder
- Right:
- Left:
50 (52.1%)
29
21
35 (36.4%)
6 (6.3%)
4
2
5 (5.2%)
2
3
51 (59.3%)
27
26
24 (27.9%)
8 (9.3%)
3
5
3 (3.5%)
1
2
Ulcer Size (cm2): *
● Mean±SD:
● Range:
19.5±12.5
0.5~99.1
21.5±13.4
7.26~61.65
Stage of the Ulcer:
● Stage I:
● Stage II:
● Stage III:
● Stage IV:
14 (14.6%)
27 (28.1%)
28 (29.2%)
27 (28.1%)
11 (12.8%)
23 (26.7%)
27 (31.4%)
25 (29.1)
Sepsis upon entry:
● Positive:
● Negative:
20 (20.8%)
76 (79.2%)
17 (19.4%)
69 (80.2%)
* Due to wide range, a non-parametric test (Menn-Whitney’s) was used (P=0.06).
All differences were not statistically significant (P>0.05).
Figure 1

Figure 2

90y, Bed sore before treatment 4 weeks after treatment 10 weeks after treatment 12 weeks after treatment
Figure 3

Figure 4

65Y, Bedsore before treatment 3weeks after treatment 6weeks after treatment 12weeks after treatment
Figures 1, 2, 3 and 4 show the progressive healing of deep (stage IV) pressure ulcers in elderly bed-ridden patients receiving MEBO. Figures 1 and 2 represent progression of healing of left trochanteric and sacral pressure ulcers respectively, in the same patient, at the same time intervals. There was a significant (P<0.05) increase in healing index (HI) (Figure 5) and reduction in ulcer surface area (Figure 6) on weeks two and four respectively, that was maintained through 12 weeks in patients receiving MEBO as compared to those receiving Fucidin. Cumulative patient sample percentage showed that 56.3% (54/96) of ulcers treated with MEBO had complete healing (HI = 1) by 12 weeks, as opposed to only 19.8% (17/86) of those treated with Fucidin (X2=15.248,P<0.001). Moreover, none of the patients receiving MEBO had a HI of <50% by 12 weeks as compared to 26.8% (23/86) of those receiving Fucidin (X2=66.271,P<0.001) (Figure 7). Linear regression analysis showed that the change in ulcer size and healing index can be attributed to ointment application (r2> 0.4). No adverse effects or hypersensitivity reactions of the ointment were encountered in either group.
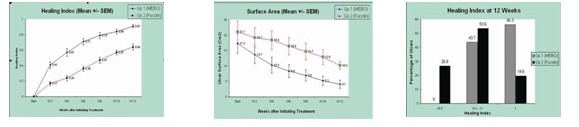
Figure 5HI with Time (weeks) Figure 6SA with Time (Weeks) Figure 7HI at 12 Weeks
3.FIGURE LEGENDS
Legends of Figure 1(a-d):A 90-year old bed-ridden gentleman with a deep (stage IV) left trochanteric pressure ulcer, on admission (Figure 1∶a) treated with MEBO and followed-up for 4 weeks (Figure 1∶b), 12 weeks (Figure 1∶c), and 18 weeks (Figure 1∶d) showing progressive and almost complete ulcer healing.
Legends of Figure 2(a-d):Deep pressure ulcer (stage IV) in the sacral area of the same patient, on admission (Figure 2:a) treated with MEBO and followed-up for 4 weeks (Figure 2:b), 12 weeks (Figure 1:c), and 18 weeks (Figure 1:d) showing progressive and almost complete ulcer healing.
Legends of Figure 3(a-d):Deep pressure ulcer (stage IV) in a 60-year-old patient, on admission (Figure 3:a) treated with MEBO and followed-up 3 weeks (Figure 3:b), 10 weeks (Figure 3:c), and 90 days (Figure 3:d) showing complete ulcer healing and patient discharged back home.
Legends of Figure 4(a-d):Deep pressure ulcer (stage IV) in the sacral area of 65-year-old patient, on admission (Figure 4:a) treated with MEBO and followed-up at 3weeks (Figure 4:b), 6weeks (Figure 1:c), and 12weeks (Figure 4:d) showing progressive ulcer healing and the patient back home.
Legends of Figure 5:Healing index (HI) of pressure ulcers in both groups with time showing significant increase of HI in patients receiving MEBO starting at 2 weeks after initiation of therapy.
Legends of Figure 6:Surface area (SA) of pressure ulcers in both groups with time showing significant reduction of ulcer size in patients receiving MEBO starting at 4 weeks after initiation of therapy.
Legends of Figure 7:Proportion of healing pressure ulcers in both groups after 12 weeks of initiation of topical therapy. Note complete healing of >50% of pressure ulcers in patients receiving MEBO.
4.DISCUSSION
Pressure ulcers greatly affect the lives of patients and their family caregivers. These effects include physical, emotional, social and financial status; change of body image; and loss of independence and control[16]. Despite technological advances that have given a myriad of options for managing pressure ulcers, the effective, practical, and affordable local wound care modality does not seem to be available yet. Nevertheless, the preferred modality should be one able to maintain moisture over the wound surface, preserve cytokines and growth factors present in wound exudates, provide an effective barrier against bacteria and external physical factors, facilitate debridement when necessary, and reduce pain. Reduced cost, and practicality of dressing application and maintenance in position are also factors to be considered.
It has long been known that a moist environment facilitates wound healing more so than allowing the wound to air dry[4~6]. Therefore, any dressing that does not provide the necessary moisture for wound healing should be disregarded except probably when dealing with infected wounds in which the moist environment would exacerbate the infection[3]. Several studies provided some evidence that hydrocolloid dressings were better than saline gauze or paraffin gauze dressings for complete healing of chronic wounds[17]. Adherent wet-to-dry (saline) dressings, low adherent wound contact dressings and perforated film absorbent dressings do not seem to be appropriate for the management of chronic open wounds healing by secondary intention. On the other hand, foam dressings, polysaccharide dressings and alginate dressings do not provide as such the optimum moist environment for healing unless combined with a secondary synthetic adhesive moisture-vapor-permeable (SAM) dressing which by itself is labor intensive and impractical to use over large surface areas and difficult to maintain over certain anatomical areas. Likewise, hydrocolloids, hydrogels, and the new hydroactive preparations though capable of providing the proper moisture, require the same secondary dressing for positioning. MEBO, on the other hand, produces the adequate environment for moist wound healing without the need of any cumbersome, elaborate or expensive secondary dressing[3].
In the present study, we compared MEBO dressing versus Fucidin for the local management of chronic pressure ulcers. The active ingredients of MEBO are ?-sitosterol, flavinoids (mainly baicalin), alkaloids (mainly berberine), in a base of bees wax and sesame oil. Such active components provide the physiological moisture for optimal wound healing by facilitating keratinocyte migration, angiogenesis and interaction with growth factors[3]. Moreover, such ingredients allow MEBO to be effective through the three known stages of wound healing; by providing rapid autolytic debridement (first stage), facilitating the development of good and healthy granulation tissue (second stage), and facilitating re-epithelization with no hypo- or hyper-pigmentation (third stage).
The present randomized clinical study showed the simplicity, safety and efficacy of MEBO in local management of chronic pressure ulcers. Significant increase in healing index of any given pressure ulcer is to be expected as early as two weeks following initiation of treatment. Atiyeh et al[18] reported similar results in their multi-center prospective study. Although there was no control group in their study, yet it clearly showed that MEBO may induce rapid reduction in ulcer size even after a stagnant state with other therapeutic modalities. When a healing plateau is reached, additional therapy mostly surgical debridement and soft tissue coverage becomes indicated whenever feasible. If surgery is not an option as dictated by the patient’s age, underlying pathologies and associated diseases, ointment application can be continued for prolonged periods of time without leading to the emergence of resistant bacterial strains while maintaining the wound in a relatively clean and socially acceptable condition. On the other hand, various creams, ointments, powders, or solutions available for use as topical anti-microbial agents may control bacterial growth at the wound site for some time, but in most cases, will definitely not cure infection[19]. Indiscriminate use of these agents for prolonged periods of time may predispose to the emergence of resistant strains and several may cause skin hypersensitivity reactions or may have an adverse effect on wound healing[20].
Occlusive dressings prevent surface desiccation greatly enhancing re-epithelization and wound contraction, and reduce also pain during the healing phase[21]. However, early occlusive dressings were quickly abandoned because of the potential of bacterial proliferation and their difficulty of application in areas other than the extremities[22~23]. In addition, Duoderm (Convatec), a new type of occlusive dressings that keeps a moist non-adherent environment over the open wound[22], has been associated with the formation of granulomas with increased inflammation and potential scarring[24]. Further, when occlusive dressings are used on large surface areas, the amount of dressing exudate becomes unmanageable and it becomes cost ineffective and labor intensive[25].
A new concept in local wound management applicable to chronic ulcers is the negative-pressure wound therapy (NPWT). It is primarily designed to prevent exudate collection while simultaneously preventing desiccation of the wound. It has also been claimed that these dressings increase oxygen tension in the wound, decrease bacterial count, increase granulation formation, and prevent shear force on the wound surface[26]. Additional advantages include diminished need for daily dressing changes enhancing patient’s comfort, decreasing nursing work, and probably diminishing cost of wound care. Though the principle is basically simple, applying this type of dressing does require certain expertise and may not be applicable to all types of wounds, such as those with inadequate circulation, fibrotic, desiccated and devitalized wounds with eschar, in addition to wounds that are too small to allow the NPWT foam dressing to come into contact with the wound bed[27].
Based on the results of this study it may be concluded that, in addition to its simplicity and safety, MEBO dressing significantly promotes the healing of chronic pressure ulcers with significant increase in the healing index of any given pressure ulcer starting two weeks following initiation of treatment, and complete healing of more than 50% of the ulcers by 12 weeks. Another comparative study between this topical treatment modality of chronic pressure ulcers and other existing practices particularly NPWT merits further investigation.
References
[1]Cuddigan J, Ayello EA, Sussman C, editors. Pressure Ulcers in America: Prevalence, Incidence and Implications for the Future. Reston, VA:NPUAP, 2001:25~48.
[2]Robson MC. Can acute wound healing be accelerated? Contemp Surg 2000, 12~13.
[3]Atiyeh BS, Ioannovich J, Al-Amm CA, Al-Musa KA. Management of acute and chronic wounds: The importance of moist environment in optimal wound healing. Current Pharmaceutical Biotechnology 2002, 3: 179~196.
[4]Svensjo T, Pomahac B, Yao F, Slama J, Erikson E. Accelerated healing of full thickness skin wounds in a wet environment. Plast Reconstr Surg 2000, 106: 602~612.
[5]Al-Musa KA, Sawwaf A, Dham R. Scar quality and physiologic barrier function restoration following moist and moist exposed dressings of partial thickness wounds. Dermatologic Surg 2003, 29: 14~20.
[6]Atiyeh BS, Al-Amm CA, Nasser AA. Improved healing of split thickness skin graft donor sites. J Applied Research 2002, 2: 114~121.
[7]Xu R. The medicine of burns and ulcers, a general introduction. Chinese J Burns Wounds Surf Ulcers 1989, 1: 68.
[8]Li L. Experiment on inhibiting constriction of the ileum from a white mouse. Chinese J Burns Wounds Surf Ulcers 1990, 2: 50~51.
[9]Xing D. Experimental study on the actions of the moist burn ointment on promoting healing of skin wound and anti-infection. Chinese J Burns Wounds Surf Ulcers 1989, 1: 76~77.
[10]Geng XL, Bu XC, Gao FQ, Liu YL. Study on the bacterial count of variable tissue of burn wound. Chinese J Burns Wounds Surf Ulcers 1989, 1: 49~50.
[11]Huang QS, Zhou G, Su BP, Huang EX. A comparative study of fibronectin and MEBO in the treatment of experimental rabbit corneal alkaline burn. Chinese J Burns Wounds Surf Ulcers 1995, 7: 18~27.
[12]Wang GS, Jian WG, Xu XS, Lang QX, Zhang XS, Wang KQ, et al. The exploration of pathological changes and their mechanism of experimentally burned rabbits after treatment. Chinese J Burns Wounds Surf Ulcers 1992, 4: 7~11.
[13]Atiyeh BS, Ghanimeh G, Kaddoura IL, Al Amm CA, Ioannovich J. Letter-to-the-editor, Split thickness skin graft donor site dressing: Preliminary results of controlled clinical comparative study of MEBO and Sofra-tulle. Ann Plast Surg 2001, 46: 88~89.
[14]Erikson E, Perez N, Slama J, Page CP, Andree C, Maguire JH. Treatment of chronic, non-healing abdominal wound in a liquid environment. Ann Plast Surg 1996, 36: 80~83.
[15]Bergstrom N, Bennett MA, Carlson CE, et al. Treatment of Pressure Ulcers. Clinical Practice Guideline, No. 15. AHCPR Publication No. 95-0652, Rockville, MD: Agency for Health ‘Care Policy and Research, Dec 1994.
[16]Langemo DK, Melland H, Hanson D, Olson D, Hunter S. The lived experience of having a pressure ulcer: a qualitative analysis. Adv Skin Wound Care 2000, 13: 225~235.
[17]Barclay L. consensus statement describes dressings for acute and chronic wound management. Arch Dermatol 2007, 43: 1291~1294.
[18]Atiyeh BS, Ioannovich J, Magliacani G, Masellis M, Costagliola M, Dham R. The efficacy of moisture retentive ointment in the management of cutaneous wounds and ulcers. A multicenter clinical trial. Indian J Plast Surg 2003, 36: 89~98.
[19]Debbasch C, Brignole F, Pisella PJ, Warnet JM, Rat P, Baudouin C. Quaternary ammoniums and other preservatives’ contribution in oxidative stress and apoptosis on Chang conjunctival cells. Invest Ophthalmol Vis Sci 2001, 42: 642~652.
[20]Steed DL. Treatment with growth factors and skin equivalents. Contemp Surg 2000, 17~22.
[21]Vogt PM, Andree C, Breuing K, Liu PY, Slama J, Helo G, Erikson E. Dry, moist, and wet skin wound repair. Ann Plast Surg 1995, 34: 493~499.
[22]Reuterving CO, Agren MS, Soderberg TA, Tengrup I, Hallmans G. The effects of occlusive dressings on inflammation and granulation tissue formation in excised wounds in rats. Scand J Plast Reconstr Surg 1989, 23: 89~96.
[23]Feldman D, Rogers A, Karpinski R. A prospective trial comparing Biobrane, Duoderm, and Seroform for skin graft donor sites. Surg Gyn Obstet 1991, 173: 1~5.
[24]Nemeth AJ, Eaglstein WH, Taylor JH, Peerson LJ, Falanga V. Faster healing and less pain in skin biopsy sites treated with an occlusive dressing. Arch Dermatol 1991, 127: 1679~1683.
[25]Robson MC. Discussion: Dry, moist, and wet skin wound repair. Ann Plast Surg 1995, 34: 499~500.
[26]Argenta LC, Morkwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg 1997, 38: 563~576.
[27]Subhas G. Guidelines for managing pressure ulcers with negative pressure wound therapy. Adv Skin Wound Care 2004, 17 (Suppl 2): 1~16.