- 论烧伤创面治疗原则

-
目录
- 英文摘要
- 论烧伤创面治疗原则
- 烧伤监护与临床处理第四讲 血气指标对酸碱平衡的考核(上)
- 介绍一种多功能测量体温盒
- 烧伤病房物品表面的细菌测定
- 烧伤疤痕头皮角一例报告
- 应用超薄皮瓣修复手外伤皮肤缺损及手瘢痕挛缩畸形
- 手指侧方逆行岛状皮瓣修复指端软组织缺损
- 改良软组织扩张法治疗26例疤痕性秃发
- 脐膀皮瓣在上肢高压电烧伤中的应用 (附7例报告)
- MEBO在手外伤后创面长期不愈的应用
- MEBO与PIC联合治疗单纯疱疹性角膜溃疡25例临床观察(附30例对照)
- MEBO治疗带状疱疹30例临床疗效观察
- 应用MEBO治疗鼻前庭炎46例报告
- 湿润暴露疗法治疗烧伤围休克期的治疗
- 烧伤湿性疗法抗休克临床经验体会
- 湿干性疗法对照治疗功能部位烧伤
- MEBO在194例面、会阴、臀部烧伤中的应用体会
- 浅谈湿润烧伤膏作用机理的微观学说
- 浅析烧伤医学三大要素——烧伤预防、治疗、康复
- 美国专家对中国湿润烧伤膏及烧伤湿润暴露疗法的剖析评论
- 徐荣祥创烧伤湿润暴露疗法——全美烧伤受难者基金会主席来京向徐教授颁奖
On the Principle Of Treatment of Burn Wound
Xu Rongxiang
(China National Science and Technology Centre foe burns,Wounds and Ulcers Beijing Guangming Chinese Medicine institute for Burns,Wounds and Ulcers)
Abstract
The article expounds the therapeutic features Of the MOist Exposed Burn Therapy (MEBT)in the treatment of burn injuries by means of experimental research data and clinical application experiences about MEBT and confirms that the principle and method Of conventional dry therapy for burn injuries is contrary to burn pathogensis,,while MEBT i.s an effective medical technique which is in conformity with burn pathogenesis at present.
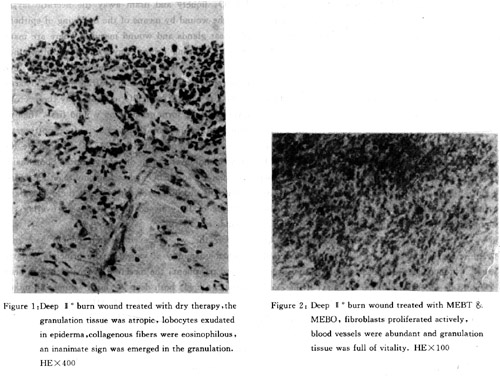
Histogical studies confirmed: microscopical examination of wound tissue treated with dry exposure therapy showed that the granulation tissue was atrophic, in which the lobocytes exudated, collagenous fibers were eosinophilous. An inanimate sign was emerged in the granulation tissue. The wound tissue treated with MEBT was full of vitality,fibroblasts proliferated actively and there were aboundant blood vessels. The comparison study be. tween amnion overlying therapy and MEBT in the treatment of superficial 11 o burnt wound confirmed that the later could make the wound heal through epidermization. The wound treated ash the former was only overlaid by 2--3 strata of epithelial cells.
Bacteriology studies confirmed:the bacterial count per gram tissue underneath the wound treated with MEBT was less than 104/g. Comparing with that of the wound in control group, P value (0. 001. Comparing with that of the wound treated with SD--Ag,P value>O. 05.
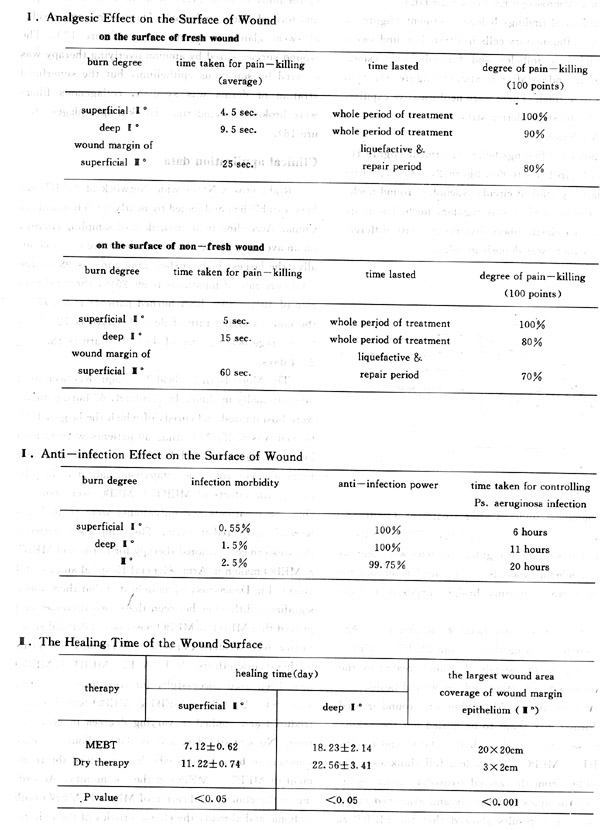
Pathological studies confirmed:MEBT could make deep II bubs wound heal with its whole derma recovery and leave no scars. The wound treated with dry therapy healed with scars. Examination under the optical microsape showed many inhemmatory cells infiltrated around the substaneous hair follicles and sweat glands and became focal before MEBT. After MEBT, epiderma returned to normal. There were 'nebforrkative capillaries and fibrob--; lasts in the dea stratum. The examination under the electronic microscope showed: before MEBT, nucleus was irc regaller with many circular vacuoles around it,having no nucleolus or irregular nucleolus. The elastic fibers of der- ma were disarranged with different thickness, chondriosome was vacuolar degeneration. After MEBT, the intercellular bridge of stratum spinosum was recovered to be normal. The shape of prickle cell was clear and regular with a clear aled regular nucleus, cating at the centre of the cell. The distribution of euchromatin was unl form. Th. clinical aPPlication of MEBT & MEBO cored: MEBT and MEBO were suitable for minor,moderate and extensive burifns, ning reliable analgesic and anti--infective effects. Deep II burn.could be cured without forming scars. Minor and moderate III burns could be healed through epidermization in a short time. The total cure rate of inpatients was 99.25 %. The total cure rate of 40% -- 80% body surface area burned patients was 89. 75 %.. The largest body surface area cured was 98%. The cured skin mean area of deep III burn through epermiztion cells of wound mare in wihtout skin grafting was 20 X 20cm. The largest of it was 35 X 20cm. In addition, the general treatment plan was established initially. Comparing with dry therapy,the minor and moderate burns could be treated by anti--shock and nutrition therapy. The fluid and protein could be supplied orally. For extensive burns, the volume of fluid infusion was cut down by 1/3. The required volume of nutrient solution was small at the early stage. The required volume of nutrient solution was relat.ively larch at the late stage.
Preface
In the 30s of this century,the dry and anti--in- fective therapy were used as the principles of treat' ment for burn wound in burn surgery field. Later on, the treatment barrier of burn wound with a BSA burnt over 30% which had lasted for thousands years was broken down by means of skin grafting technique of , surgery. Then the burn pathogenesis was discovered which has contribute to the sucessful treatment of extensive burns. Since then, the treatment system of burn surgery was formed initially in clinic and became the treatment routine for burn injuries and was applied world wide.
UP to 70s, burn surgeons were disappointed in the therapeutic results and patients' suffering. The further experimental studies made them vacillate .in theory and practice of conventional dry therapy. However, at that time no new technique could replace the conventiopal medical technique for treating burn inJuries.
In the late 70s, the author began to be involved in the burn pathogenesis research. So far a reformation of conventional dry therapy for burns has been fuL filled and the moist therapeutic system has -been established, which has been popularized throughout China and applied succes'sfully in clinic in the U. S. and countries in Middle East and Southeast Asia. Right now MEBT is spread to more and more countries. The largest body surface area burned and cured by it is 98%. Deep H o burn wound can be healed and covered by full thickness derma. The experimental studies and successful clinical application of MEBT brought about a thorough revolution in the dry medical technique. It announces that the basic theory of therapeutics of dry medical technique is wrong and its therapeutic method is wrong and unproper. The mistake points of dry medical technique are as follows:
1. The mistakes of basic theory of therapeutics:
The dry therapy deemed that the burn skin tissue of stasis zone was destined to necrosis. For preventing infection, it should be desiccated to necrosis as soon as possible. While the moist medical technique deemed that the burn skin tissue of stasis zone was able to recover completely. It should be survived and any damage to it should be abated.
2. The mistakes of therapeutic methods:
A. let the wound without epidermal protection be exposed and damaged directly by air.
B. The rule for burn treatment is regeneration and repair. Keeping wound dry can't make tissue regenerate and repair.
C. Using antibiotics topically to prevent and treat burn wound infection doesn't treat burn itself. There are 10 major injuries of burns. The bacterial infection is caused by burn injuries. So to prevent and treat burn wound infection by using antibiotics topically is only to treat the compliCation of burns and the antibiotic for external use can worsen the burn injuries.
D. Bandaging wound on pressure is wroung both in theoretical and methodological aspects. The pressure can exert negative influence upon the recovery of dermal microcirculation and exacerate cell edema and microcirculation stasis. On the other hand, the rising temperature of wound due to bandage can enhance hydration reaction and aggravate tissue injury.
E. The escharotomy and skin grafting are techniques of traumatic surgery instead of burn surgery techniques. In face, escharotomy is to excise the burn wound. The burn trauma is transfered into scalpel trauma. Then the new cut is treated by skin grafliting. So what treated is scalpel trauma but not burn trauma.
In short, for the topical tractment of burns, no matter what kind of the method is, it must tie in conformity with burn pathogenesis. The dry medical technique absolutely does not treat burns but damages burn tissue. This scientific conclusion raises the most rigour revolutionary subject before every burn researcher. Innumerable burn patients expect us to acquire medical techniques for burns as soon as possible. The author has researched the MEBT and put it into practice for more than ten years. Up to now, the new medical system has been eatablished. I would like to report some of the research achievements about this subject. This is only for the reference of colleagues around the world.
A brief introduction to MEBT
MEBT is a kind of burn therapy designed according to traditional chinese medicine and modern medical . science. MEBT realizes its therapeutic actions with the coordination of MEBO. The characteristic of MEBT's action is to make the burn tissue expose to a three dimensional moist environment, which conforms with the physiological condition, in order to facilitate . necrotic tissue discharge, regeneration and repair. The technique standards of MEBT:
A. Keep wound moisturized but not macerated.
B. Liquefy and discharge the skin necrotic layer from superficies to interior.
C. Fulfill the adequate drainage from inter--tissue to outlayer of wound surface by means of MEBO.
D. Guarantee to burn tissue the steady supply of active ingredient of drug with constant concentration and draining off from wound surface, through its dosage form and other actions.
E. isolate the wound from air irritation and damage and meanwhile discharge the excreta or metabolite of wound timely. After the above 5 major effects act on the wound simultaneously, MEBT can realize its therapeutic effects. The Joint actions of MEBT and MEBO is referred to as Moist Burn Medical Science. Its clinical therapeutical features are summed up as follows:
a. To relieve wound pains by ways of non-- anes-tlhtesia.
b. To prevent add control infections by non-- bactericidal or non--bacteriostatic ways.
c. To alleviate the progressive necrosis of burn : wound by the moist environment and pharmaceutical action of MEBO.
d. To make deep II burn wound healed without scaring by creating a physiological environment for skin regeneration. The datails about its features of therapeutic effects on extensive burns will not be referred to in the article.
Treatment method: Smear MEBO on the burn wound directly to a thickness of about 0. 5--lmm. According to above mentioned technique standards, control the opportunity for next application of MEBO untill the wound is healed up completely. Before MEBT, In general,it's not necessary to sterilize or debride the wound. For serious contaminated wound, it can be irrigated by clean water, then suck up the water by gauze and apply MEBO on the wound. The liquefied substance can be cleared away by gauze of tissue or by tongue depressor at liquefaction period.
Data of experimental studies
1. histological experiment.
A. Choose 14 white rabbits, weighing 2-- 2. 5 kilograms, no strict to sex. After skin preservation, the back bf each animal was scalded to form a deep 11 o burn with an area of I cm2. Then the rabbits were divided into two groups randomly. Control group was treated with dry therapy, experimental group was treated with MEBT. 18 days later, the burnt wound . tissue was sampled and examined under optical microscope.
Results: the exam of histological section of control group. showed that the granulation tissue was atropic, lobocytes exudated, collagenous fibers were eosinophilous. An inanimate sign was emerged in the granulation tissue (figure 1)
The exam of histological sections of experimental group showed that the fibroblasts proliferated actively, blood vessels were abundant and granulVion tissue was full of vitality (figure 2).
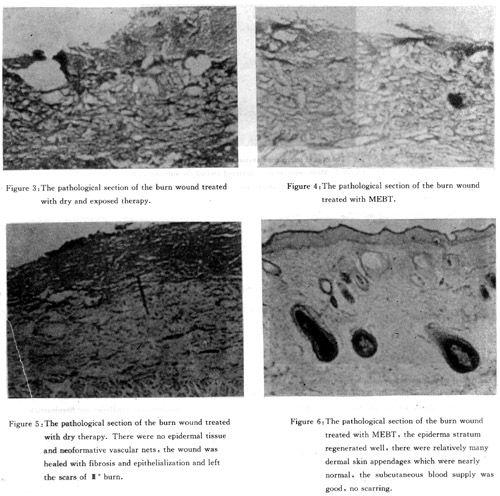
B. Choose 14 adult, healthy white guinea pigs, for each of them, cut dorsum hair and scald both sides of the back to form two deep E o wounds 2cm in diameter. The two wounds of each animal were divided into two groups randomly. In control group, the wound was treated by dry exposure therapy. In experimental group, the wound was treated by MEBT. 6 days after scalding, the wound tissue of some animals in both groups was sampled, and pathological sections was prepared. The examination under optical microscopl con firmed the burn injuries reached in deep derm; stratum. (figure 3,4). The rest of the guinea pigs received treatment continuely until the wound was recovered. Then sample the healed wound tissue, prepare pathological sections and examine them. The resuits showed the wounds in control group healed witl scars. While the wounds in experimental group healec with the recovery of full thickness derma structure. (figure 5, 6)
2. Bacteriology studies
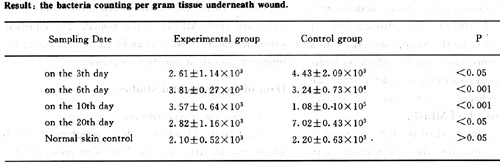
A. Choose healthy guinea pigs. For each animals, cut the dorsum hair and scald both sides of back to form two deep I o wounds at random. One wound was treated by dry exposure therapy, the other was treated by MEBT. The animal were killed in 4 batches, 7 animals in each group. The tissue underneath the wound surface was sampled and the becteria counting was conducted.
B. Select 120 healthy wistar white rats, weighing from 100-- 200 grams, no strict to sex, cut the dorsum hair of the aminals, scald the back of them to form each a N o burn wound with 20% BSA burnt, then paint lml of previously prepared 4x108 PS aeruginosa suspesion on the whole burn areas and divide the white rats into four groups as follows.
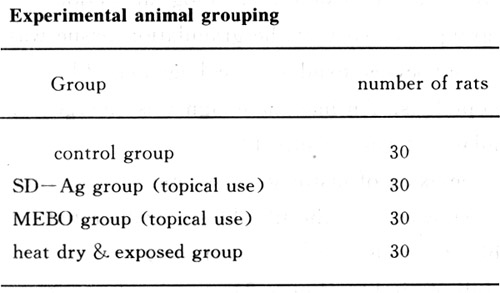
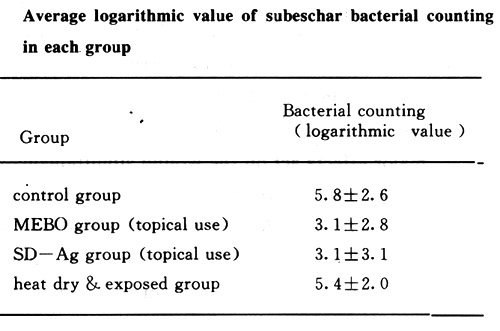
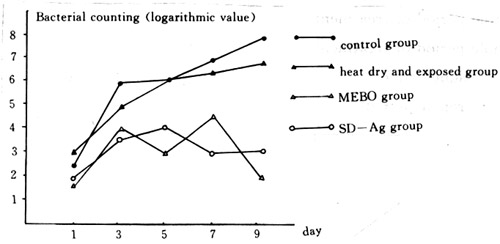
animals in each group were treated by corresponding therapy. Six white rats were killed respectively 1, 3, 5, 7, .9 days after treatment under aseptic manipulation. The living tissue underneath the wound was sampled and the bacterial counting in it was conducted. The average logarithmic value of each group's bacterial counting of subeschar living tissue showed that the average value of bacterial counting of MEBO group and SD--Ag group were obviously less than those of the control group and heat dry & exposed group. The difference between groups was statistically significant (P < 0. 01 ). There was no significant difference between heat dry & exposed group and the control group (P>0. 05). There was no significant difference either between MEBO group and SD--Ag group (P>0. 05).
the following graph illustrates the relatiottship between bacterial counting of subeschar tissug: and the course of the disease in each group.
3. Pathological Observation
A. The disunion III burn wound after skin grafting was treated with MEBO in clinic. Then, the treated wound tissue was examined under the miciroscope and transmission electronic microscope (TEM) and etc.
Optical Microscope Exam: (X 200HE)
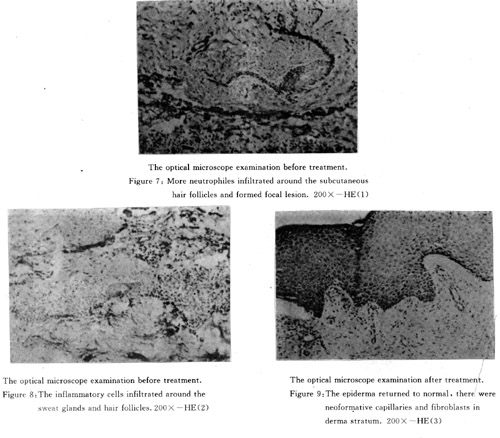
Pathological findings before treatment (figure 7, 8, 9): The inflammatory cells infiltrated around sweat glands and hair follicles and formed focal lesion. Pathological finding after treatment (figure 9): Skin returned to normal. There were neoformative capillaries and fibroblasts in derma stratum.
TEM. Exam:
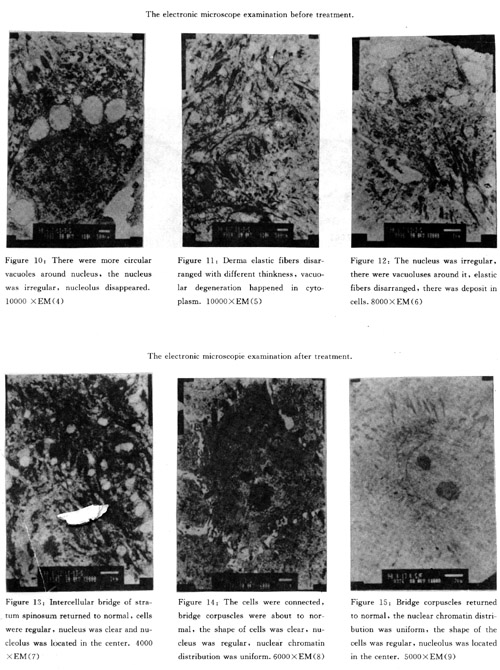
Pathological findings before treatment (figure 10, X 10000, figured, X 10000, figure12, X 8000): There were relatively a lot of circular vacuoles around nucleus, the nucleus surface was regular, nucleolus disappeared,derma elastic fibers disarranged with different thinkness, there was deposit in cells.
Pathological findings after treatment (figurel3, X 4000, figure14, X 6000, figurels, X 5000): Cells of stratum spinosuhi were regular, nucleus was clear to be seen, nucleolus was also clear, nuclear chromatin distribution was uniform, bridge corpuscle became normal.
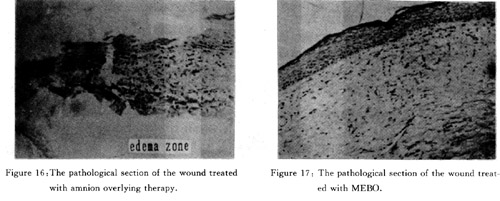
B. The disunion superficial III wound was treated by amnion overlying therapy and MEBT & MEBO in clinic. The derma islands of wound treated by the latter connected each other and the wound healed two weeks after treatment. Meanwhile the wound treated by the former was about to be healed but the asking thin.kness was thinner than that of the wound treated by MEBT & MEBO. 1 X 0. 4cm full thinkness skin was sampled from the wound treated by aboye mentioned two 'therapies respectively and examined under microscope. The results showed that the MEBT & MEBO cured wound surface was overlaid by squamous epithelium, cells in every stratum Were well ranged and formed a new epidermal. There were some residual sweat glands in derma tissue (figure 17 ). The wound surface cured by amnion overlying therapy was covered by squamous epithqlium, but the superficial stratum of derma was swollen, collagenous fibers were broken, no epiderma and skin appendages (figure 16 ).
Clinical application data
Right now a Nationwide Network of MEBT has been established and joined by nearly 4000 hospitals in China. According to statistic data of sampling survey,on an average, 150000 burn inpatients are cured annually, the largest body surface area cured is 98%, the total cure rate of inpatients is 99. 25%, the total cure rate of 40% -- 80% BSA burned patients is 89.75%, the non-scarring rate of deep E o burn is 72.25%, the average healing time of deep II burn is 18. 23 + 2. 14 days.
The Moist Burn Medical Technique has been used internationally in clinic. In Thailand, 67 burn patients were hospitalized and cured, of which the largest BSA burned was 85%. Meantime 30 patients were treated by SD -- Ag in General Hospital of Royal Thai Air Force as a control. The comparison indicated that the therapeutic effects of MEBT & MEBO were remarkable. 58 inpatients and outpatients were treated and were all recovered in Syria. The comparison between the western conventional therapy for burns and MEBT & MEBO maken in Army General Hospital and Capital Hospital in Damascus, Syria indicated that there was a significant difference between these two therapies and proved that MEBT MEBO possessed a decided superiority over Western Conventional Therapy for Burns in therapeutic effects. In U. A. E., MEBT & MEBO have been used successfully for treating post --burn scars, etc. UP to now MEBT & MEBO have been introduced and applied in varying degrees in 28 countries. No statistic data are available about the case numbers of burn victims who have received the treatment of MEBT & MEBO in the community. According to the clinical application of MEBT & MEBO both at home and abroad, the characteristics of their thera peutic effects can be summarized as follows:
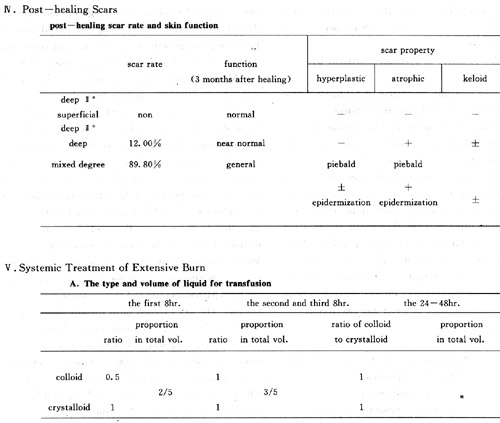
The total volume of transfusion: the first 24hr is 0.8ml every l% BSA burnt per kilo weight physiological requirement. If urine output is normal, then plus 2 times of physiological requirement. The second 24hr is 0. 7ml every 1% BSA burnt per kilo weight + physiological requirement. If urine output is normal, puls 2 times of physiological requirement. (2 time physiological requirement includes physiological requirement. )
B. The principle of treatment at shock stage
a. Slow down the velocity of transfusion when the body temperature returns to normal ;
b.. Slow down the velocity of transfusion and cut down the;transfusion volume to fit the physiological requirement when urine output become normall
c. Slow down the transfusion velocity and use cardiotonic when body temperature is beyond normal, urine output is normal or beyond normal and heart rate is in excess of 120/per min. (except for heart rate rising due to high body temperature).
d. Stop anti--shock treatment and transfuse fluid according to urine output when shock symptoms are recovered.
c. The principle of nutritive and supportive therapy.
The nutrition therapy of low nitrogen and high calorie is applied before liquefactive period. The ratio of nitrogen to calorie is 1: 200 X 6. 8. The nutrition therapy of high nitrogen and low calorie is applied at wound repairing period. The ratio of nitrogen to calorie is 1: 100--150 X 6. 8. Early nutrition supply through digestive tract is encouraged. Taking food and other nutrition as early as possible is good for the patients.
Formula of the total calorie supplied: namely the physiological requirement of calorie every day + calorie requirement of burn wound BSA every day, that is weight (bio. ) X 25 X 6. 8 joule + BSA% deep burned X 20 X 6. 8 joule.
D. The principle of systemic treatment by using antibiotics
a. Avoid systemic application of antibiotic if possible for treating moderate and minor burns
b. Advocate early use of ordinary dosage of broad --spectrum antibiotic which will not cause organ damage such as penicillin and erythromycin.
c. New type antibiotic can be used systemically for a short period of time (3 -- 5 days) for extensive burns of burn patients who suffer 'from serious septicemia. Stop using it if the therapeutic result is not satisfactory and turn to use broad--spectrum antibiotic with which will not cause organ damage ordinary dosage. Meanwhile strength nutritive and supportive therapy and immunotherapy, protect organ functions and maintain the balance of water and electrolyte.
Discussion
The Methodology of Burn Studies and Therapeutic Effect Evaluation of Burn Treatment
There are several thousand therapies for burn injuries throughout the world, including overlying ther- apy in which more than three thousands covering materials are applied. However, since there has been no unified standard for therapeutic effect evaluation in the world so far, it is difficult to come to a common idea in determining which therapy is a satisfactory one among the huge number of therapies for burns. The author's research offers a general idea and reminds people to re -- question whether the basic theory of therapeutics of the former local therapies for burns is right and is the burn local therapy in conformity with the burn pathologic law through the objective fact therapeutic effects. According to the research results, the author expounds and proves the basic theory and method of local burn therapeutics from the angle of methodology research.
I. Expound the Principle of Burn Wound Treatment on the Basis of Life Law
Burn injuries is the damage of body surface, it's a kind of ischemic damage. its pathogenetic period can be described simply as burn necrosis necrotic tissue sloughing residual tissue regeneration repair. The treatment aims at removing the' putrid tissues, promoting the growth of new tissues and restituting vitality. So the study of the local treatment of burns should base on regpneration and repair. To violate this principle me against burn therapeutic law. All burn therapies which violate this principle are harmful to the surface of burn wound. Thus the correct method of burn study is established, namely to study the resurrection and regeneration of burn tissue. There are general biotic laws for all vital bodies with vital activities: the growth law, the senility and death law,and revival law. The burn local pathogenesis is no exception to these laws. Provided that our research methods tally with the above mentioned biotic laws, We can ensure the soundness of research methods and gain the therapies and medicines which are in line with the burn pathogenic law and favourable to burn wound healing. The dry exposed burn therapy (DEBT) is a destructive therapy for burn injuries, it hinders vitality, so it is a wrong way of treatment. The local application of antibiotics is for the purpose of controlling bateria growth, since it holds back the regeneration of cells at the same time, it violates the revival law. So the local use of antibiotics is unsuitable.
II. Expound the Principle of Burn Treatment on the Basis of Bioconditions
The burn tissue bioconditions are that of skin tissue. The closer the vital conditions created by the effects of therapy are to skin tissue biocondition, ado matter what kind of therapy it is, the correcter the principle of burn treatment is. The epiderma of normal skin protects the skin tissue from harmful effects of natural environment, the micro -- blood circulation network of normal skin supplies the tissue with oxygen and carries metabolite, the tissue fluid produces moistness and growth environment for tissue cells, the skin appendages adjust the general system in addition to its effect adjusting the function of skin tissue. The burn injuries destroys the normal environment sustained by skin tissuse, so out therapies have to compensate for skin biocondition damage and help the maintenance of skin bioconditions. MEBT can take such compensation and maintenance effects. On the contrary, DEBT, bandaging therapy and water bath therapy destroy the vital condition of skin tissue. Their mistakes can be pointed out in airi water content and temperature, these three aspects. After epiderma is peeled off and derma is damaged due to any injuries, the oxygen and nitrogen in the air will react directly on skin tissue and cause oxidizing and azotiz. lug reaction. As a result the tis~ cells are dead abruptly. So we can say that after being burned, the skin tissues suffer from another damage --air damage 9 which is nearly the same to burn damage itself. Since DEBT treats burn wound by means of air, it is a b' wrong and destructive therapy. While MEBT isolates burn wound from air and provents it from air damage effectively. As for water content damage, because it is tissue fluid who sustaines the moist environment of . tissue, rather than H2O, any therapy increasing or decreasing H2O is destructive to physiological moist environment of tissue's own. DEBT causes wound tissue much dehydration, on one hand, tissue is desiccant and necrotic, on the other, a lot of tissue fluid exudates from wound tissue, blood circulation volume reduces. In result shock gets worse, water--electrolyte balance is disturbed, a great quantity of heat and protein is lost. MEBT is a kind of anhydrous treatment, it can prevent water loss and maintain the physiological moist environment of tissue through sebum like funtion of MEBO. The water bath therapy is absolutely different from MEBT in theoretical basis, it is alctually a refurbished version of DEBT. In fact, it brings about burn wound overhydration, exacerbates . tissue edema, causing hydropic damage. So water batlys therapy is a destructive treatment as well. The temperature damage exists widely in current therapies such as bandaging therapy, infrared radiation therapy and varied membranous overlying therapies. After burning, the residual and chemical heat cerated by burns still remain on wound and/or continue to release to burn tissue, which lead to accumulative heat, producing further accumulative heat damage. MEBT predvents and relieves accumulative heat damage effectively through the actions of MEBO's dosage form. On the contrarly, DEBT, oven dry therapy and infrared therapy all belong to the treatment which worsens the accumulative heat damage of burn tissues. For ban'daging therapy under pressue can raise burn wound temperature, it reinforces hydration reaction of wound surface and aggravates burn wound injuries.
III. Expound the Principle of Burn Treatment on the Basis of Histophysiology
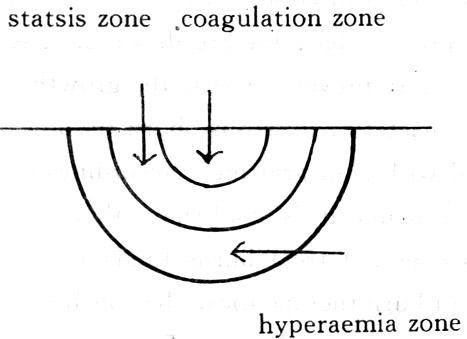
There are three concentric injury zones in burned areas from superficies to interior of wound. The tissue in the superficial injury zone has already been necrotic and is unable to recover, the lowest or deep injury zone is called hyperaemia zone, the tissue cells in it have inflammatory degeneration and will be recovered within several days, so it is also called recovery zone, The zone between surface and deep injury zone is statsis zone, the tissue cells and microcirculation in it are in a state of "half--deadll and in a state of prsgressive thrombosis respectively. From the above histophysiological changes of burn tissue, we can find out that the key to burn wound treatment is to treat the zone of stasis. The medical science of dry therapy for burns is convinced that the histophysiological changes of stasis zone are unreversible. The tissue and microjcirculation develop into rtecrosis gradually, during this period, the bacteria are easy to breed and the wound is infected, finally causing septicemia which is dangerous to life.
In its therapeutics, three major principles of treatment are established and applied based on above mentioned point of views. 1. Make static tissue in the zone of stasis dried and crusted as soon as possible so as to prevent bacteria breedingl 2. Use high power antibiotic to prevent or stop the growth and reproduction of bacterial 3. Excise burn tissue early and treat wound with skin grafting. According to its principles of treatment, it is confirmed that dry therapy for burns does not treat burns fundamentally. From the angle of burn therapeutics. the conclusion can be made that it is a wrong therapy; From the angle of general therapeutics. the conclusion can be made that it is a destructive therapy aiming at saving life of burn patients.
Starting with painstaking studies of burn pathogenic law the Moist Burn Medical Science is convinced that the histophysiological changes of static tissue are reversible. The tissue and blood circulation
can be gradually recovered totally or mostly. Thus a medical science direct opposite to dry burn medical science is established. The research and treatment of dry burn medical technique focus on how to enhance the death of burn tissue, while that of moist burn medical technique focus on how to promote the recovery of burn tissue.
The Moist Burn Medical Technique resolves following problems effectively:
A. The transition from half--dead histiocyte to normal.
B. The transition from inflammatory cell to non --inflammatory.
C. The transition of histiocyte from pathologic picture to physiologic.
D. Eliminating the four main causes of progressive microcirculation stasis, the reduction of blood flow velocity, hemoconcentration, bad micrangium structure and endangium changes, speeding the recovery of microcirculation. Thereby the principle of treatment, the therapy and the drug which conform to burn pathogenesis and treat burn injuries itself effectively are developed. Because the basic theory of therapeu. ties of dry medical technique is wrong, it is impossible for the principle of treatment, therapy and drug based on it to produce any effective therapeutic actions ; it is a totally wrong local therapy.
IV. Anti--wound infection Should be Favourable to Wound Healing
The treatment of burn wound bacterial infectior should be favourable to wound healing, this is t.he es. semials of treatment, for the goals of anti --infection and treating burns are the same--to promote healing. However the current conventional therapies and drugs for burn wound infection go against this repairing law of burns. They unilaterally place the emphasis only on one point of the treatment, especially Consider that to use antibiotic is to treat bums. Thus the difficult problem--anti--wound infection has not been solved. How to treat burn wound infection and enhance or not interfere wound healing at the same time? Let's has an analysis by means of biological law.
A. The advantages and disadvantages of using antibiotics:
It is important to treat bacterial infection with antibiotics, but this refers only to the general bacterial infections. Is the situation the same for bacterial infection of burn wound ? We can find out the answer only in the pathogenic law of burn wound infections. There are about 1000 bacteria in per gram normal skin tissue, which indicates that the bacteria also involve in skin physiological activities. his impossible for skin to regenerate in an environment without bacteria existing. When burning happens, the bacteria and skin tissue in zone of coagulation are burnt, away together, the bacteria in zones of stasis and hyperaemia are damaged to the same degree of the skin tissues in the relevant zones. After burning, the bacteria change along with the pathological changes of burnt skin tissue. This is the vital law of the normal bacteria staying in derma tissue. In addition, the exogenetic bacteria coming from intestinal tract, respiratory tract and environment etc. aggregate on the surface of wound, reproducing and causing wound infection. According to above laws of bacterial production and infection, we know that the environment change of wound tissue happens at first, then the bacteria stay on the wound and reproduce. So the principle of infection treatment is to adjust the conditions of tissue environment first and then to control the bacterial reproduction.; It will always be in a passive position to control bacteria only. The principle of conventional treatment puts emphasis on application of antibiotic. It only considers the latter situation and therefore it is one--lsided. Do the advantages outweigh the disadvantages or otherwise if the wound is treated by antibiotics ? The initial conclusion can be made through above analysis: the disadvantages outweigh the advantages. It will be ily understood by analysing the pathogenic process of wound. It seems that it is effective to apply antibiotics only on the burn wound at the period of inflammatory reaction, but it is wrong to use antibiotics at the repairing period of wound because that the actions of antibiotics aim at preventing and inhibiting the develop ment of nil fen. Antibiotic inhibits the regeneration of histiocytes when it sterilizes bacteria or inhibits bacterial growth. It preventsthe recovery of burn tissue at the period of inflammatory reaction, stops the repair of burn wound at the period of wound repairing. In Oct. 1990, when the author was invited to Thailand to, rescue the burn victims, he was asked to hold a consultation at one of the army hospitals. A doctor there asked: The BSA and degree burned of the patient we treat are the same to that of the patient you treat, but why does the wound of the patient you treat heal up and while the wound of the patient we treat turn to granulation state gradually after the necrotic tissues have discharged from wound? The author asked in reply:What kind of the drug you have used to trea.t wound? The doctor answered:n SD -- Ag cold cream. 11 The author asked again:II What is the effect of SD--Ag cold cream?" The doctor answered: n Its effect is to sterilize Ps. aeruginosa and other bacteria." The author asked:n Does SD--Ag have the effect of promoting cell regeneration?" The doctor replyed:n No, it doesn't. n Then the doctor said with smile: I see, SD -- Ag is not a drug of promoting skin growth. It inhibits the tissue regeneration when it sterilizes bacteria."
B. How to promote wound healing and control bacterial reproduction as well.
The statement in paragraph A has pointed out the pathogenesis of bacterial infection. There are four wsys to adjust the physiological environment of wound based on bacteriology research: 1. to kill bacteria; 2. to inhibit bacterial 3. to perish bacteria; 4. to treat bacteria with body's autoimmunity. According to vital law of wound, since the immunologic function of wound's own is low, it is difficult for wound itself to treat bacteria with its own immunity. The anti-- infection action of wound's autoimmunity can realize initially with the help of phagocytizing bacteria action, temperature, PH value, water content, oxygen supply, drainage and bacteriaal respiratory condition etc. In fact, such an immunologic environment is favourable to recovery and regeneration of tissue and unfavourable to growth and reproduction of bacteria. The anti --infection action of MEBT designed by the author is just produced through these links. Bacteriological research data of this report show that MEBT can creat the same anti--infection effect as that SD-Ag does without through the way of sterilizing bacterIa.
V. To Promote Wound Healing is Essential to Burn Treatment
Burn is the summation of all traumas. Its pathogenesis results from body surface burn, so to treat burn wound is fundamental to burn treatment. However, the conventional burn therapy does not treat burn due to its mistake of treatment direction. How to treat burn wound ? The author has made achievements of burn wound treatment in the researches of burn traumatology and repairing science.
After burning, the damages of skin may be summed up as following ten kinds of damage:
1. residual heat damage;
2. air damage
3. dry or wet damage;
4. autochemical damage
5. edematous pathologic damage
6. microcirculation damage of stasis zone;
7. static damage of tissue
8. damage of tissue's rejection reactionl
9. damage of histiocytes' disintegrative products
10. iatrogenic damage.
There are 5 major pathophysiologlL changes in the repairing process of burnt skin:
1. the damage, inhibition and resuscitation changes of histiocytes
2. the emergence of foundation of derma microcirculatory vascular network and the establishment of vascular tree
3. the establishment of myoblast function and collagenous fiber structrue
4. the regeneration and repair of residual skin appendages: hair follicle sebaceous and sweat glands and their excretory ducts
5. the establishment and regeneration of epiderma stratum.
So to evaluate whether a therapy really treats burn tissue, we should determine whether it is effective to 10 major damages and 5 major pathophysiologic changes, otherwise it does not treat burn really.
The dry medical technique for burns has no therapeutic effects on above mentioned damages and pathophysiologic changes fundamentally, on the contray, it worsens damage and stops regeneration and repair. The moist medical technique for burns has therapeutic effects on above mentioned damages and pathophysiologic changes fundamentally, thus it gains satisfactory effects clinically.
The action characteristics of MEBT in the treatment of burn wound:
A. Directed by MEBT, MEBO is smeared on the wound and the residual heat and its damages are eliminated as the dosage form of MEBO transfers from o.intment to liquid state.
B. The wound is isolated from air and survived from air damage because of MEBT, the two state distribution of MEBO on the wound and drainage action of MEBO on the wound.
C. Since the dosage form of MEBO is anhydrous lipoid substance, its function is close to that of sebum, it can keep wound moisturized but not macerated and desiccated.
D. MEBO contains relatively powerful anti--inflammatory substance (wound ulcer substance) which can inhibit the chemical substance release of tissue after burning.
E. MEBT owns adequate drainage action which makes exudate not stagnate ic dead space. MEBO contains medicinal plant ingredients (5--sitosterol etc. ) which have an action of promoting blood circulation by removing blood stasis, so ac subside the tissue edema greatly.
F. MEBT & MEBO stop the 4 major causes of microcirculation stasis damage satisfactorily, namely to abate the hemoconcentration of local blood vessles due to its preventing visible and invisible dehydration; to increase local blood flow and speed up the velocity of blood flow by its active ingredients; to maintain and ,protect the integration of vital vascular structure due to its stablizing cell membrane and relaxing smooth muscule 1 to prevent and relieve local blood coagulation reaction effectively due to its adequate drainage action and inhibiting the release of inflammatory substances and anti--platelet aggregation action
G. MEBT & MEBO improve the local microcirculation, stablize the histocyte membrane and improve the condition of local oxygen supply, as a result, lessen tissue's static injury.
H. 5--sitosterol of MEBO has a strong anti-- inflammatory action, it prevents the inflammatory reaction as well as abates the rejection reaction.
I. Examinations under the optical and electronic microscope show: MEBT & MEBO not only make inter, tissue metabolite and excreta,be drained away . macroscopically by means of the physical and chemical changes of MEBO's base but also effect the marvelous changes in histiocyte fine structure such as the abnormal connection of cell desmosome transforms into normal oned nucleus from irregular turns to regular; irregular chromosome becomes regular one and other normal physiologic transformations of cell organs.
J. MEBT & MEBO are not damaging therapies, thus they will not cause any iatrogenic injuries.
The action characteristics of MEBT & MEBO in the process of burn wound repairing:
A. Make the damaged local histiocytes which are in an inhibitory state resuscitate 16-- 24 hrs ahead of time.
B. Liquefy and discharge the necrotic layer from superficies to interior which is favourable to the retention of residual. vascular foundation, ensure the total establishment of vascular trees due to non pressure, non covering and three dimensional moist physiological environment throughout the period of treatment. This environment is also beneficial to myoblasts' syntblesizing celluloses and the natural arrangement of collagenous fiber structure.
C. Keep the exudate of residual glandsi be discharged from wound tissue constantly in the whole period of wound repairing because that MEBT tis a moist and exposed therapy and MEBO's base is a sebum like substance, as a result, guarantee the entirely regener,ation of residual glands and reconstruction of excretory ducts of glands.
D. The author discovered in experiments that MEBO enhances the synthesis velocity of DNA and RNA in derma epithelial cells which cuts down the mitotic cycle to several times to ten time of normal one.
The author has not referred to any other medicines and therapies for burn wound reported in internationl medical magazines which owns the action characteristics of MEBT & MEBO analysed and summarized above. MEBT & MEBO are the only technique and medicine in the world nowadays which really produce the therapeutic effects on burn injuries.
VI. The Deep II Burn is not Doomed to Heal with Scars
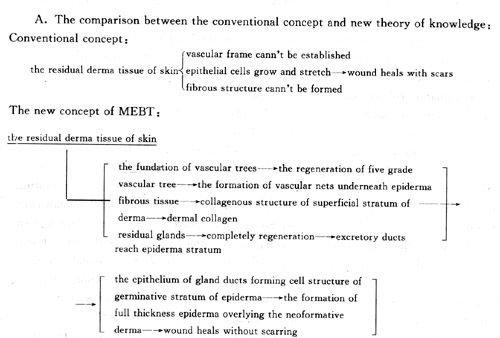
For many years the medical textbooks throughout the world all read:" There are three modes of healing of burn wound after part or most of the derma are burned.
1. The residual dermal epithelial cells of wound grow and stretch to the surface of wound directly along the subeschar, wound is healed with hypertrophic scars
2. The wound is covered by derma islands and granulation tissue after the burned skin layer peels off and autografting is needed. After the wound is overlaid by skin grafts or dressing is changed for many times, the wound heals up with scars due to skin grafting.
3. The early eschartomy and skin grafting are performed, the wound is healed with scars. n These authoritative conclusions have fostered doctors generation alter generation. It seems that nobody doubts of these generallly acknowledged conclusions. So far there are hardly any articles in international science publications negating the aforementioned conclusions. It has been considered as a categorical truth and an unalterable fact that deep n o burn will be healed with scars. the author's researches confirm that deep II burn is not doomed to heal with scars but completely recovered with full thinkness derma which has also been proved by the author's colleagues after repeated experimental studies and a lot of clinical practice. The author's achievement negates the above mentioned conclusions fundamentally and therefore a new healing standards of deep II burn are established.
B. The delllnonstration of basic theory of histology:
The burn histology studies bring to light the general : law of burn scar formation. It can be summed up as follows: the original tissue of acarring: fibrous tum of subcutaneous tissue; the vascular nets of dermal underlayer ;the residual dermal glands and tissue of gland ducts. The experimental research findings: the residual dermal tissue underneath the stasis zone is in an inhibitory state after the most of the derma are burnt. 4 days later the survival tissue begins to resuscitate, on the 7th -- 10th day after burning, the survival tissue and necrotic tissue start to reject and separate each other, meanwhile the residual histiocytes begin to regenerate and repair.
a. the change of fibrous tissue: the myoblasts produce a lot of fibrocytes 9 the majority of them are collageous fibrocytes. Their velocity and quantity of growth are several times or dozens times of that in the repairing process of ordinary trauma. In the epithelia] cell regeneration period of ordinary trauma, a fibrous cell can regenerate 4 cells, the ratio is l: 4, while the ratio in burn repairing period is 1: 20. The more important finding is that the maturation rate of fibrous cell of ordinary trauma is high, that of burn injuries if low. The researches of dry therapy and moist therap indicate that the direct maturation rate of celluloses of myoblasts in dry therapy is 60%, while that of celluloses of myoblasts in moist therapy is 98%. The researches in clinical practice find out that in the dry therapy the immature collagenous fibrocytes develol into mature ones within 10-- 20days after wound healing. The cells are from thin into thick ones. In mois. therapy, there are only few immature collagenous fibrocytes which will get mature before wound healing.
b. the changes of vascular nets: the vascular networks in human derma tissue distribute as tree in fly grades. In dermal underlayer, the vascular distribunon is the 3rd vascular trees which is parallel to skil surface. The derma injury means to cut off the vascu far trees at their top, trunk and hasal parts. The re construction of vascular trees means the regeneratiol of vascular trees by residual vascular trees growinj from the damage plane which are similar to norma vascular trees. The researches prove that because thl dry therapy destroys the regeneration environment the vascular trees can not regenerate in accordancl with their original structure but grow disorderly an form vascular balls. While the moist therapy create the regeneration environment for vascular treed makes the vascular trees regenerate in accordance with their original structure. Finally the repairing of dermal vascular trees is fulfilled.
c. the changes of epithelial tissue: After the derma is injuried, the epithelial tissues in the residual derma tissue are a tiny quantity of sebaceous glands, sweat glands of derma underlayer and their excretory ducts, hair follicles and epithejium of hair follicle stem. All of these epitheilial tissues come from ectoderm and therefore have the common heretitary characteristics. Even through their functions are different, they all have the histology basis of forming epiderma. Both epithelial cells of hair follicle stem and epithelium of sweat gland excretory ducts have the physiological function of hasal layer cell of epiderma and can fully regenerate epiderma. The glandular cells can transform from secretory hasal layer cells of epiderma into non--secretory ones. Even through this law has been recognized for nearly a century, the burn therapies applied destroy the ecological environment of epithelial cells and make the residual epitheliun unable to regenerate completely. In dry therapy, since the crust restricts the completely regeneration and repair of epithelial, the epithelial tissue and body of gland can not regenerate completely when the burn wound is healed. The moist therapy complies with the regeneration of epithelial tissue and makes the already incomplete epithelial tissues and glands of derma regenerate and repair completely.
Vll. The Exploration of Principle of III Burn Wound Treatment
It is well known that III burn wound is easy to treat but there is no satisfactory therapy for it. As for damage degree, the burn tissue has lost the treatment opportunity because of the full thickness skin n.ecrosis. So in order to save life, the eschartomy and skin grafting are performed. So far no satisfactory therapy is available for extensive III burn wound. According to pathogenic studies, the III burn wound is grouped into two types, one is the full thickness skin necrosis with fatty layer injury the other is the necrosis of full. thickness skin and fatty layer with nuscular layer injury. According to the characteristics of damage, the wound can be divided into directly damaged burn wound and progressively damaged III burn wound.
The four injury characteristics above can be observed in all early burn patients in clinic. Thus the general impression produced by III burns is that since there is no skin left,how to get the skin. However, according to above mentioned pathogenic features, it doesn't mean that there is no outlet for III burn wound. The following is the analysis based on experiences in clinical treatment:
The former clinical experiences showed that the skin grafting should be considered for III burn wound with a diameter over 2cm;early eschartomy or reserying eschar and skin grafting should be performed for extensive III burnsl the early eschartomy and skin grafting should be performed for profound deep III burn wound which may develop into III burn wound; etc. All of these principles of treatment are produced on the premise of saving patients' life. In fact, treatment is not given absolutely to III burn wound. Therefore we should do research to find out whether there is possiblity of treating III burn wound. The author demonstrates the feasibility of the treatment of III burn wound in the light of change law and damage intensity of III burn tissue.
A. Part of the III burn can be prevented early; According to the theory of stasis zone and pathological changes of three injuried zones of burns, if the tissue of derma underlayer develops into necrosis, the wound is a kind of III wound with fatty damage. The opper.." tunny and method of treatment are still available for this kind of the wound. The pathological changes of sttasis zone is a dynamic process and have their own clluses. After fatty layer is injuried, the skin sources are still available, since there are a lot of sweat gland epithelia in fatty tissues. So the principle of treatment ; is to prevent and treat progressive necrosis of tissue of stasis zone and to cause the epiderma regeneration making use of residual epithelia of sweat glands. This conclusion has been proved in clinical practice. The 1. \ concerning pathological data are published in this article.
B. The small area III burn wound (20cm in diameter or less than) with muscular layer damage treated with MEBT & MEBO can be healed naturally right now. The wound margin epithelia of epidermal hasal layer can regenerate, stretch to overlay wound surface. The skin grafting of trauma surgery is still needed for extensive III burn wound with muscular damage. In the future this kind of wound may be treated by transplantation technique of epithelial cells.
C. The application of MEBT in the treatment of III burn wound: MEBT has five actions on III burn wound.
1. To relieve the profound deep III or mixed degree burn wound and prevent them from becoming III burn wound
2. To liquefy and discharge the necrotic skin, develop the sweat gland epithelia to epiderma overlying the wound
3. To impel the wound margin epithelia of III burn wound involving muscular layer damage with a diameter less than 20cm to grow, in result epithelia stretch to overlay the wound and the wound is healed. (very few reported the diameter of treated wound was over 35cm. )
4. To creat a wound environment in order to perform skin grafting and treat residual wound.
5. Coordinating with spotty skin grafting, to promote the regeneration and stretch of grafts.
Vlll. The Exploration of the Principle of Comprehensive Treatment of Extensive Burn
The treatment of extensive burns is a kind of surgical comprehensive treatment. The several major difficult problems facing the doctors and several major crises facing the patients are well known. According to the initial successful experiences gained by the clinical practitioners from our burn medical centers throughout China in the four year rescue and treatment of extensive burn patients, the author sums up the following principles of treatment.
1. The concepts of rescue and treatment: The former conventional rescue and treatment of burns stands for focusing the treatment of saving patients' life. Doctors rescue and treat burn patients at all costs and by using all therapies. Provided that the patient is survived after treatment, the great success is achieved. However, according to national conditions of China, only few patients have the chance to receive such expensive treatment. Even if they are survived and healed, few of them will lead a happy life at this heavy cost. The situation is the same in the Western countries. So they advocate that the extensive burn treatment depends on the healing results and economic conditions. In our country,the burn treatment should renbody the humanitarianism which means to heal the Wounded and rescue the dying. Meanwhile we should be practical and realistic and aim at curing the sickness to save the patient. We should consider the ways of treatment within our power according to healing effect and survival rate. Many extensive burn patients were cured before by conventional medical techniques, but the majority of them were totally disabled which brought new suffering and burden the patients,their familys and society. Under this circumstance, the principle of extensive burn treatment should be based . on curing the diseases. In order to make the survived patient become a person with certain viability instead of disabled person, what we have to consider first is the post--healing function of the patient.
2. Emergency Treatment: Whether in war or peacetime, no matter how the patients come, in batch. es or individually, the principle of emergency treatment pursued is to prevent further damages and rescue patients on the spot or at local hospital as near as possible. The early emergency treatment of burns includes resuscitation, protecting wound, managing concurrent trauma and preventing shock. Resuscitation, managing concurrent trauma endangering patient's life and protecting wound are earliest treatment and must be conducted on the spot. The burn wound is the pathogenetic source of extensive burns. So we should consider early wound protection is as im... portant as resuscitation. Since the occurrence of shock is a progressive process, comparatively speaking, its management is not as urgent as resuscitation and wound protection are. The following is the exposition o f principles of burn emergency treatment:
A. To introduce resuscitation and understand the disease conditions on the spot. For general extensive burn, after resuscitation, measure is taken to protect woundl Therapies of neutralizing toxicant and stop. ping toxicant absorption are adopted for chemical and toxic chemical burns3 Try to keep respiratory tract unobstructed for serious inhalation injury Treat the concurrent trauma endangering life, according to principle of trauma emergency treatment. As for mine burn or explosive burn, the "impact injury should be considered first. Since the impact injury has damaged the heart and other internal organs, the patient should stay in bed for fear of increasing oxygen consumption of myocardium and causing traumatic heart failure.
B. To protect wound: The wound protection in emergency treatment of burn injuries includes two aspects, one is not to produce traumatic injury on the wound, the other is to prevent injuries of natural environment and iatrogenic injury. To debride or debride thoroughly in conventional emergency treatment of burn wound is unsuitable. To sterilize and irrigate the wound is on purpose to keep wound clean and prevent infection, but in fact this goal can not be attained. On the contrary, these management cause a negative stimulation on wound and worsen the shock. Wound irrigation makes the burned skin hydrolyzed and hydrated, a lot of hydrolyzate and hydrate are absorbed which inhibit myocardial function and result in heart failure. The author maintains that the wound is treated simply on the spot, then it is band up by cloth or other suitable materials, ir MEBO is available, it can be smeared directly on the wound so as to isolate the wound early, kill wound pains and make preparations for further treatment. If MEBO isn't available on the spot, plant oil can be smeared simply on the wound. If nothing is available on the spot, the wound can banded up simply without handling wound temporarily. According to bacteriology, the burned skin is relatively clean, the bacteria in skin are burnt away as corresponding skin is burnt alive. So it is insignificant to sterilize the already dead skin after burning. Even. if the patient has transfered to hospital, we should strive to treat wound simply. The thorough debridemerllt is forbidden. The practical lessons tell us the more thoroughly the wound of the patient is debrided, the earlier the patient is dead. For extensive burn patients with impact injury, the more energy the patient consumes, the earlier the patient dies. If the wound is treated by MEBT, the treatment can contintte directely, according to methods of MEBT. If other therapies are used, simple way of treatment is advocated.
C. To prevent shock: Preventing hurl shock early is a key to successful burn treatment. The emergency treatment on the spot should be perfgrmed in the light of the principle of traumatic surgery. Attention should also be paid on the management of concurrent injury and the cause of burns. Since the pan TInt burned under mine suffers from impact injury as well, fast - and big volume transfusion are inadvisable for this kind of patient. The fluid infused can be chosen from local sources in order to maintain water --electrolyte balance. If there is no condition for trans fusion on the spot, patient can take water or soft drink.
3. The principle of wound treatment: The wound management of extensive burns runs through the whole period of treatment. After several year clinical practice, the Moist Burn Medical Science has summarized its own principle of treatment initially. The following principles should be stood for during the treatment:
A. To confirm the principle of treatment according to the deepth of burn wound: Before the deepth of bum wound is confirmed, MEBT and MEBO should be applied boldly. The protective treatment is conducted first and the wound is observed for 6 hours. If there is exudate on the wound and the wound colour turns to white after the wound reacts to MEBO,the deepth of the wound can be confirmed as over deep E o burn temporarily and then the wound is treated as deep II burn. At present, all the burn wounds with the deepth over II including the 100% BSA burnt wound are treated with MEBT & MEBO. After 6 hour observation, if there are no obvious exudation and white substance on the wound, the observation should be taken for another 6 hours, if the exudation and white substance emerge on the wound, the wound should be treated according to above--mentioned principle. But for the wound whose BSA burned is over 80%,the thickness of MEBO has to be adjusted timely in the light of patient's general conditions. The biger the BSA burned is, the thiner the drug layer is. After 12 --hour observation, if there are no exudation and whital substance on the wound, and the patient has not suffered from burm shock yet 9 the wound can be diagnosed as III burn wound.
B. The principle of III burn wound treatment:
In clinic, the III burn wound has two healing modes, for minor burns, the mode is to heal by means of the epitht,lia stretch of sweat glands and wound margin; For extensive burns, the mode is dependent on patients' vital conditions. Conservative treatment can be adopted for superficial III burn wound whose TBSA burnt is less than 50%. The treatment of III burn wound whose BSA burnt is over 50% has to draw support from techniques of traumatic surgery so as to close the wound. Therefore, what we have to continue to study is the treatment of extensive III burn wound. So far the principle of necrotic layer treatment of III burn wound has not been unified yet. For minor and moderate III burns, Doctors have basically reached unanimity of opinion: Make use of MEBO, liquefy and drain away the necrotic layer, cure the wound by means of the overlying of epithelia of sweat glands and wound margin. There are many ways of treating necrotic layer of III burn wound, some doctors stand for reserving eschar first, then performing excision and skin graftingl some advocate that: Use MEBT & MEBO to clear away the necrotic layer and help form granulation wound first, then do skin grafting and cure the wound or after spotty grafs have survived, use MEBT & MEBO to promote the growth and development of spotty grafts. Some maintain that: Use MEBO and eschartomy together to discharge the necrotic layer and then let the sweat gland epithelia of fatty tissue or grafted skin overlay the wound. etc.
On the whole, even though people have not reached unaminity of views on the principle of burn wound treatment, the direction of treatment has been unified, namely both deep n o burn wound and mixed burn wound are treated with MEBT & MEBO, no matter that it is extensive burn or minor one. The treatment of extensive m o burn is based on the goal of function recovery at later stage.
Summary
The article fully demonstrates the correctness of MEBT & MEBO in the treatment of burn injuries based on experimental researches and clinical application data and points out the therapeutics mistakes of dry medical technique theoretically and practically. By means of the demonstration of principle of burn wound treatment, the author aims at appealing medical practitioners to undertake the important task of reforming medical techniques of burn wound and to be involved in the revolution era of burn medical science.
The writer also points out subjects concerning burn injuries which need further researching. Since this article is too long, the comprehensive treatment of extensive burns will be demonstrated eleswhere.
References
1. Fang Doughal "Clinical Application and Experimental Study of the Moist Exposed Burn Therapy"《The Chinese Journal of Burns Wounds & Surface Ulcers 》 1989,l,P. 29
2. Chen Xiaowu, et al. "A Comparative Study of the Effects of Moist Burn Ointment, Silver Sulfadiazine and Hot Exposed Therapy on Controlling Pseudomonas Aeruginosa infection of Burn Wounds 《The Chinese Journal of Burns Wounds & Surface Ulcers》 1990, 3,P. 39
3. Zhang Xuezhong “ Electron Microscopy of One Case of Skin Burn Wounds Treated with MEBO ” 《The Chinese Journal of Burns Wounds & Surface Ulcers》1992, 2, P. 6
4. Chen Shirui “ Effect of the Moist Burn Ointment in l Case of Extensive Burn ”
《The Chinese Journal of Burns Wounds & Surface Ulcers 》 1989, 1, P. 44
MEDIA RELEAST
MEDIA RELEASE CHINESE MOIST EXPOSED BURN OINTMENT/THERAPY ANALYZED BY U. S. EXPERTS
Beijing, May 13, 1993-- Harrys. Gaynor, Chairman and President of the National Burn Victim Foundation, U. S. A.., made the following statement at a press conference at the Beijing Hotel:
During November 1989 1 visited China to learn about claims made by professor Xu Rongxiang of a revolutionary treatment for burn injuries. Both Dr. Anthony Barbara, a podiatric burn surgeon from the U. S. who accompanied me, and I examined a number of burn patients in Beijing and Dalian, all of whom had sustained moderate to critical injuries.
Prior to visiting Professor Xu in Beijing we were not convinced that the reports about his ointment and methodology were for real. After spending ten days visiting patients and learning about the methods applied in treatment, we were convinced that we had observed a revolutionary breakthrough in the medical management of burn treatment.
In 1990 and again in 1992, Professor Xu visited the United States and lectured to physicians specializing in burn treatment at hospitals in Washington. DCI Cincinnati, Ohio; Bethesda, Maryland, MassachusettsF New York and New Jersey. Generally the physicians were interested in learning more and were.receptive to clinical tests in the U. S.
To expand of knowledge of Dr. Xu's methodology, I brought with me to China two weeks ago Dr. Peter Fan, a U. S. surgeon and medical specialist, and Dr. Walter Robey, a U. S. surgeon specializing in the emergency treatment of trauma. Both Dr. Fan and Dr. Robey were skeptical about MEBO and MEBT, Professor Xu's burn ointment and methodology. Howevd, after observing patients being treated with MEBO. I believe I can safely say they are no longer skeptical. It is clear to me that what I have seen with my own eyes is indeed a revolutionary breakthrough in the treatment of burns.
Every day in hospitals around the world, children and adults are suffering from painful burns and are at risk of life threatening infection of their burn wounds all needlessly, in my opinion. Needlessly, because there appears to be a far better way for treating burn injuries discovered in china by Professor Xu Rongxiang.
It is frustrating to me and my associates at the american National Burn Victim Foundation when red tape and physicians who will not accept change cause delays in bringing this new technology quiCkly forward to save lives, reduce morbidity and shorten me hospital stay of burn patients.
From our observation, this revolutionary burn m6thodology is extremely cost effective. The staggering costs of burn treatment in the United States could be significantly reduced if Professor Xu's methods were utilized today. I am sure that if all hospitals in China were using as techniques and ointment, not only would burn patients benefit, but a significant reduction in the cost of hospitalization would be attained.
I am encouraged after visiting hospitals in China that are treating burns in the Western methods have now partially or fully changed their protocol for -burn treatment.
It isn't easy for physicians to change to a new way of treating patients. Only through education and the development of scientific data will doctors worldwide accept change. So let us get on with what must be done to serve the humanities. Let both medical disciplines join together to cooperate in upgrading the treatment of burns.
I have seen the pain and hopeleSsness on the faces of numerous burn patients in the United States and in other countries who were being treated with western burn treatment. What is amazing is the healthy appearance and smiles we have seen on Chinese burn patients when treated with MEBO.
It is vital that health agencies responsible for the health and care of those who suffer from burns and other surface wounds take positive steps to incorporate this new methodology into their research and clinical testing programs and to begin to take positive steps today for the sake of those who are and will be suffering and dying needlessly.
If I were to be granted a last wish in my life before I die, it would be that doCtors who practice western burn methods and those using the moist exposed burn therapy (MEBT) would join together in their mutual interest to benefit mankind in this critical area of trauma.
I am delighted to announce today that professor XU Rongxiang has agreed to join American interests in a formal agreement of cooperation to begin the necessary steps to bring his revolutionary ointment and treatment methods to the United States to seek US Food and Drug Administration approval. It is our opinion that Such an approval will become a reality. We are also encouraged by the committment of Professor Director General Ma Junru, Director General of the State Bureau of Foreign Experts toward bringing together the interests of China and the United States in this revolutionary, life saving treatment for burn injuries.
SUPPLIED BY:Mr.Harry J.Gaynor,President
National Burn Victim Foundation,USA