- 英文摘要

-
目录
- 英文摘要
- 烧伤病人的多死因统计与死亡链分析
- 烧伤病人自身抗体检测及其临床意义
- 电损伤的治疗进展
- 急性呼吸窘迫综合征
- 湿润烧伤膏治疗成批大面积烧伤的护理
- 烧伤湿润暴露疗法治疗大面积烧伤病人的护理
- 大面积烧伤湿润暴露疗法休克期护理
- 湿润烧伤膏治疗26例溃疡临床报告
- 湿润烧伤膏在肛周脓肿切开术后的应用
- 湿润烧伤膏治愈慢性窦道2例报告
- 湿润暴露疗法治疗眼烧伤78例临床分析
- 湿润烧伤膏治疗骨裸露创面的疗效观察(附8例报告)
- 湿润烧伤膏治疗深部疮疡一例观察报告
- 一例特重烧伤晚期应用湿润烧伤膏治疗的体会
- 应用湿润烧伤膏治疗一例特大面积烧伤的救治体会
- 湿润暴露疗法治疗小儿烧伤72例报告
- 应用湿润暴露疗法治疗中小面积烧伤125例的体会
- 湿润烧伤膏在门诊应用(附82例报告)
- “MEBO”用于烧伤创面的疗效观察
- 湿润暴露疗法治疗烧伤191例临床报告
- 湿润暴露疗法治疗烧伤的体会
- “MEBO”在灭火现场烧伤患者中的应用
- 基层医院成批大面积烧伤的抢救体会(附“5.19”烧伤病人抢救经过)
- 湿润暴露疗法治疗烧伤面积98%的临床体会
- 首届颁发中国烧伤创疡科技进步奖
- 中国政府赴泰国烧伤医疗队救治烧伤取得成功
Clinical Experience of Treating the Burn wound on A Burned Patient of 98% TBSA With MEBO
(Abstract)
Long Jiachong Ma Enqing Liu FaZhu Zhoug Keqin Xie Youfu
(Department of Burn and Plastic Surgery, The First Affeated Hospital of Hunan Medical University )
It was reported that the successful experience in treating burn wound on a patient of 98% TBSA by means of the Moist Exposure Burn Ointment (MEBO) and Moist Semi-exposure therapy in this article. The result showed that the Moist Semi--exposure therapy not only could be used on the wound of extensive burns. but also could preserve the wound to avoid drying and infection and could promote the wound to heal up through supplying the wound with moist enviroment. liquidizing the necrotic tissues, draining and isolating the wound. It is a good therapy of treating burns. Talking about the Full--thickness burns, we consider that once the eschar of burn wound is shed and the fresh granulation is formed, the skin--grafting should be performed as early as possible in ordor to shorten the period of treatment.
The advantages and method of moist semi--exposure therapy was also introduced in the a rticle.
Experience in Treating Groups of Large Area Burn n.Patients in Grass--roots Hoseital
(Abstract)
Pn Zhuyu et al.
(Dept. of Surgery, People's Hospital, Xinbuang County, Hunan Province)
31 victims of gum powder explosion in passenger train had been treated. 10 of them were hospitalized. The treatment is summarized as follows:
I. Establ ish:ment of Organ iiing Setups :
1. Rapid establishment of a leading group.
2. Division of work and personnel arrangements.
3. Taking measures to ensure safety.
4. Strenthening cooperation.
II. Personnel Arrangements for Rescue :
1. Nurses:(1) NuTsing group. Recording body temperature, respiration. pulse. blood pressure. intake and output volume, etc.
(2) Treating group. Performing treatment and observations.
2. Doctors : (1) Group for observing ill condition, Case history, making rounds to visit patients and making instructions, writing case report and making rescue plan as the case changes.
(2) Operating group. Incision of vein for those difficult to puncture and other surgical operations.
(3) Transporting group. To carry patients into or out of the operating room.
III. Rear Service Admin istration:
1. Strenthening material supply and administration.
2. Rearrangement of the meal time and house--work time for the working personnel IV. General Data:
1. 26 males and 5 females. age range : 19 to 51, burn area 71--93% average burn area 60.27% all had head and neck burns. most of them had respiratory tract burn. 22 cased with 3rd degree burn with an average area of 12.13%, 31 cases with deep 2nd degree burn with an average area of 36.74% 31 cases with superficial 2nd degree burn. average area 17.6 % .
2. Treatment and Cause of Death.
Antibiotics were applied after hospitalization and infusion of liquids to maintain circu lation volume. Different amounts of colloids and crvstalloids for different cases.
Early treatment of wound surface. Wash with saline, clear away the sheded skin and foreign substances and apply MEBO. Cause of Death. 8 cases died in 96 hours and another case died in 6 days. The largest burn area was 93% and the smallest 53% average 69.3% all due to progressive respiratory failu re and cyanosis.
Later on 12 patients were transferred to other places for treatment. 10 patients continued to stay in our hospital. Among them 9 males and 1 female. 2 cases with burn area 60--82% 4 cases 40--59% and 4 cases 30--39% superficial 2nd degree accounted for 28% deep 2nd degree 52% and superficial 3rd degree 20% The patients were treated with MEBO and symtomatolytic therapy. The patients were urged to train with their joints. All the patients healed with no incidence of septicemia. Patients with superficial 2nd degree burn healed in 10--15 days and those with deep 2nd degree burn. 20--25 days. Those with 3rd degree burn healed in 40 days.
V. discussion:
1. Superiority of the socialist system.
2. For severe burns attention should be paid to prevent shock and changes in respiratory tract at the early stage. At the middle and later stage attention should be paid to the changes in internal organs.
3. MEBO has good efficacy and good analgesic effect. It promotes the healing pf the wound. It demands no special facilities and is suliable for use in grass--roots units.
The Application of MEBO in Treating Burn Victims at the Scene of the Fire
(Abstract)
You Judo
(Medical Team of Fire Brigade, Zhenjiang City)
Fire fighters and other personnel are always burnt at the scene of the fire. In the past. they had to be sent to the hospital for treatment. They may miss the oppotunity of being timely treated and this may lead to disablement or even death.
The author treated 37 cases of burn at the scene of the fire. during the period of August 1989 to April 1990. using M EBO to get very good resu its. This paper describes the method and detailed procedure of first aid at the scene of the fire, including how to smear the MEBO. how to treat chemical burns. eye burns, electrical bums and severe compl ications.
The results prove that MEBO has good analgesic and anti-infective effects. It improves microcirculation and prevents the deepening of the wound. MEBO is easy to be applied and is suitable for use in grass-roots units and even in fire trunk. MEBO is a necessity for every family and grass--roots unit.
Experience with MEBT in Treating Burns
(Abstract)
Guo Zkelltao et al.
(People's Hospital, Lahoou City)
In July 1990, the authors used MEBT for treating burn patients. The results were very satisfactory. The therapy is simple and has high efficacy. It is not expensive and patients need not to endure much pains.
The data of the treatment of 15 cases are .summarized as follows:
I. Clinical Data:
11 adults and 4 children(7 males and & females). largest burnt area 35% and smallest 2% 2 cases had been infected when hospitalized..
II. Treatment:
After debridement, MEBO was applied once every 4 hours. For 3rd degree burn, the necrotic tissue was excised to promote liquefication. Care must be taken to avoid bleeding, pain or injury of the heathy tissue. Patients with burn area exceeding 20% had to be infused to prevent disorder of the function of the heart, lung and kidney.
III. Results:
All the patients healed without being infected. The 2 cases already infected when hospitalized had their infections controlled. No skin graft Was needed. The shortest healing time was 4 days and the longest 34 days. No scar left for superficial and deep Znd degree burns. A case of 3rd, degree burn healed with scar but no contracture and had good elasticity.
IV. Experience:
1. Good analgesic effect. 2. Good antiinfective effect. 3. It promotes healing of the wound. 4. It reduces exudation and evaporation of the fluid and improves microcirculation and thus decreases the volume of infusion. 5. The therapy is easy to be carried out and needs no special facilities.
Clinical Report on 191 cases of Burn Treated with MEBO
(Abstract)
Qiao Haibin
(The Clinic of Neke Children's Welfare Center)
This paper reports 191 cases of burn treated in our clinic from Nov. 1988 through June 1990. The patients were treated with MEBO to give very satisfactory results. The therapy has the advantages of good drug stability, high efficacy, quick alleviation of pains, no need of analgesics, no infection and quick control of the infection already occurred and no scarring for deep 2nd degree burns. The drug promotes local blood circulation, reduces the exudate of the wound, thus greatly reduces the volume of infusion and helps the patients pass the shock and infection stages peacefully. For treating superficial 2nd degree burns. no strict sterilization is needed. The treatment may be done even at home.
Emcacy of MEBO for Treating Burn wounds
(Abstract)
Tu Wanmu
(Dept. of Burns, People's Hospital, Macheug City, Hebei Province)
The author treated burn patients with MEBO and catechol tincture respectively. The tincture was prepared by the author himself which promotes the formation of scab. The author compared the results and concluded that MEBO was much better than catechol tincture. The difference in therapeutic effect was very significant (P<0.01 ). MEBO has analgesic and strong antiinfective effects. For deep 2nd degree burns no scarring will occur. The author recognized MEBO the most ideal drug for treating burns.
MEBO Used in Outpatient Department
(A Report of 82 Burn Cases)
(Abstract)
Qiu Xiaoping
Moist exposed therapy is an ideal method for treating burns. This paper analyzes 82 cases of small area burn. A discussion on the mechanism of the therapy and the application of MEBO is presented. The author concludes that moist exposed therapy has analgesic and antiinflammatory effects. No skin grafting and no special facilities are needed, It is convenient for use in grass--roots of in ics such as in factories and mining areas.
125 Cases of Medium and Small Area Burns Treated with MEBT
(Abstract)
Li Wenlai et al.
(Dept. of Burns, Xiangtang Hospital, Haicheng City Liaoaing Province)
252 cases with small and medium area burns had been treated with MEBT. All the patients healed with no scar and good functional recovery. The following is a summary of the experience in treating 125 cases.
I. General Data:
82 males and 43 females (2:1), among which 47 infant babies.and the rest adults. Age ranged 3 months to 84 years old. Cause of burnt heat scalding accounted for 89.6% Largest burn area not exceeding 30% 66 cases with superficial 2nd degree burn healed in 7.72 days(average). 44 cases with deep 2nd degree burn healed in 18.9 days. 15 cases with mixed degree burn healed in 32.3 days.
II. Treatment:
After debridement, the MEBO was smeared on the wounds. For 2nd degree burns the smearing was a little thinner than for 3rd degree burns. The interval of applications. of the ointment was prolonged as the exudation had reduced. After 10--15 days. the wounds became smooth and epithelial islands could be observed under a magnifying glass. Gauze smeared with MEBO was applied once every day. 6 days later, the wounds all healed. After followed--up for 3 months no scarring was found. The recoverV of function was very good.
III. Conclusion:
MEBO has good analgesic and strong antiinfective effects. It promotes healing of the wound with no scarring and good functional recovery;
72 Burned chndren Treated with MEBT
(Abstract)
Pn Zhibiao et al.
(Burn Wounds and Surface Ulcers Medical Center, Yanzkou Mining Bureau)
Children burns are difficult to heal and have high mortality. The authors treated 72 burned children with MEBT. The results had been satisfactory.
I. General Data; 45 males and 27 females, age range & months to 12 years.
54.2% of the children were 1 to 3 years of age.
II. Causes of Burn; 68 cases scalded by hot liquid (54.2%).
III. Burned Area: The largest burned area was 70% of body Surface and average burned area 14.59% 26 cases had 3rd degree burns. The largest 3rd degree burn area was 6.4% average 3rd degree burn area 8.18% According to seventy. 19 cases were not severe cases. 24 cases with medium seventy, 16 cases were srious and 13 cases exceptionally serious.
IV. Results: 68 cases healed. 1 case with small burn area discharged early. 3 cases died (4.17%). 2 out of the 3 died of septicemia and 1 case died of multiple system organ failure.
V. Discussion : 1. When MEBO was applied the healing was very quick. No scar had been left for deep 2nd degree burns. 2. Perineum burn when treated with MEBO no infection occurred. 3. The volume of intravenous infusion was only 3/4 of that required in conventional exposed therapy.
A Case of Exceptionally Large Area Burn Treated with MEBO
(Abstract)
Yuan Haojun
(Dept. of Burns, Handang County Hospital, Hebei Province)
A middle aged woman with burn area of 80% deep 2nd degree 50% and superficial 2nd degree 30% and complicated with respiratory tract burn was hospitalized one hour after burnt, in a shck state. After antishock treatment, she passed the shock stage smoothly. For short of drug Supply. MEBO was applied only on the upper limbs and the rest of the burn wounds was treated with sulfadiazine silver. After two weeks, deep 2nd degree treated with MEBO had the wound surface dissolved and the skin islands fused together in 4 weeks. The residual wound surface was treated with reticular and stamp--shaped skin grafting and all healed leaving no scar. The function was very good. Won nds treated with su if ad iazine silver was followed by skin grafting. The wounds healed after scabs dissolved.
Experience:
1. After medication. attention should be paid to prevent disablement.
2. MEBO is very easy to be popularized. It is especially su liable for use in grass--roots u n its.
3. It is a necessity for modern family. It has no toxic or irritative effect. It is very effective for treating superficial medium and small area burns. No scar wilI be left.
MEBO for Treating a Case of Exceptionally Severe n Burn at the Later Stage
(Abstract)
Scan Guixiang et al.
(Debt. of Burn, Hospital of the Dalian Ckeforal industrial Co.)
In May 1989. our department treated a case of exceptipnally severe burn with MEBO. Early excision of scab, skin grafting, covering the eschar in the four limbs with allograft of large skin. Application of MEBO started on the 53rd day. The result was unexpectedly satisfactory. 17% of the superficial 3rd degree burn wounds healed spontaneously. After 6 months. pathological examinations proved that the skin had complete appendages. The wound of finger amputation ending with exposed bone had also well healed. The victim with 92/77 large area burn had been saved.
MEBO for Treating Wounds with Bone Exposed
(Abstract)
Chen Cunfu et al.
(91 Hospital)
This paper reports the short term therapeutic effect of MEBO for treating & cases of won nd with bone exposed. The largest area of bone exposure was 5 x 2.5cm2 and the smallest 3 x 1.2cm2. The longest period for healing was 62 days and the shortest 38 days, giving an average of 47.87+9.65 days. The therapeutic results had been very satisfactory. Moist therapy for treating wound with bone exposed has the following advantagest 1. No osteotomy and no skin grafting is needed. 2. It is easy to be carried out and can be applied in family wards. 3. The exposed bone and the wound are always kept moist, no bleeding due to desiccation will occur. 4. All the patients heal spontaneously, no infection of the granulation and no edema will occur. 5. The parabiotic tissue on the edge of the wound is protected, thus facilitates the growth of the epithelia. 6. After healing. the wound surface is very smooth and has a normal color. The feeling function of the skin is well recovered.
Clinical Analysis of 78 Cases of ophthalmic Burns
Treated with MEBT
(Abstract)
Wang Dexing
(China Burn Wounds & Surface Ulcers Lonhkou Scientific Madal Center)
Ophthalmic burn accounts for a great part of face burns. The result of the treatment may give a life time influence to the patients. The author treated 78 cases of ophthalmic burns of various causes, using MEBT to give very good results. it has the efficacy of relieving pains, eliminating edema and increasing lacrimation. thus protects the eye by keeping adequate drainage. Healing time had been shortened and healing rate raised.
2 Cases of Chronic Sinusis Treated with MEBO
(Abstract)
Yuan Yumin
(Surgery Dept., Traditional Chinese Medical Hospital, Chengwu County, Shangdong Province)
The author treated 2 cases of chronic sinusis using MEBO to give satisfactory results. One case suffered from chronic sinusis in breast for & years. The other infected after intragluteal injection and did not heal after incision for 3 months. After sinusis debridement and application of MEBO every other day. the patients healed in 20 and 30 days respectively.
Application of MEBO After Incision of Perianal Abscess
(Abstract)
Liu Taishen et al.
(Dept. of Surgery, Urban Central Hospital, Laiwu City Skangdong Provicne)
The authors used MEBO for treating wounds after incision of perianal abscess. MEBO gauze strips were used to keep the drainage adequate. After the wounds became shallow, the ointment was applied directly on the wounds. The authors compared the results of 32 cases. They found that patients treated with MEBO gauze strips healed in 161 days. while patients treated with old method healed in 231 days. The healing time had been markedly shortened. Pains had been alleviated: and inflammations quickly eliminated. The result of using MEBO gauze strips had been very satisfactory.
Clinical Report on 26 cases of ulcer Treated with MEBO
(Abstract)
Zhou Jingli et al.
(Dept. of surgery, Hospital of Oil Construction,Oil Field of Henan Province)
14 females and 12 males. aged from 30 to 68.with ulcers due to various causes had been treated in August 1988 through August 1990. The largest ulcer area was 6% of body Surface with a depth reaching the periost and the smallest 2% of body surface. Satisfactory results had been achieved by treating with MEBO. Two exemplary cases had ulcers for 6 months and 4 months. They were cured in 20 and 15 days after treated with MEBO 4 times every day locally. The author concluded that the drug helps to improve local microcirculation. prevent infection and promote active drainage, thus it facilitates healing of the wound. The drug is very efficacious and is suitable for use in grass--roots units.
Experience of Nursing at the Shock Stage of Large Area Burns Treated with MEBT
(Abstract)
Hua Ronglan et el.
(Nanyang Medical Center of Burn Wounds & Surface Ulcers, Hospital of the 2nd Petroleum Machine Factory)
The authors treated large area burn patients with MEBT and the experience of nursing at the shock stage had been reported.
I. General Nursing Practice :
1. Early debridement, infusion and smearing of MEBO to alleviate pains, to prevent infection and to decrease evaporation.
2. Keeping the won nds warm.
3. Keeping respiration unobstructed.
4. Establishing veinous infusion passage.
5. Urethral cathaterization.
6. Stomach tube for those with gastrectasis and enteroparalysis.
7. Physical sign observation.
8. Oral administration of MEBO for those with esophageal burn.
9. Patients allowed to lie on back, but not to face downwards, at the shock stage.
II. Infusion:
Infusion should be done in a planned way. Attention should be paid to the changes in urine volume, blood pressure, pulse and mental state. III. Artificial Hibernation : Drugs used for artificial hibernation should not be mixed with other drugs of basic property and should be used only after the blood volume had been restored. After the patient felt asleep the drug should be given more slowly. Avoid transpotation during the h ibernation period.
Nursing Experience in Treating Large Area Burn Patients Nursing Experience in Treating Large Area Burn Patients with Moist Exposed Therapy
(Abstract)
Dai Haiping
(People's Hospital, Xichuang County, Hunan Province)
In last May, our hospital treated 10 patients with large area burn due to gun powder explosion in passenger train, using. moist exposed therapy. All the patients healed.
I. Clinical Data : 5 males and 1 female, age range 19 to 48. 4 cases with total burn area 30--39% of body surface, 4 cases 40--59% and 2 cases 60--82% 7 cases complicated with respiratory tract burn. superficial 2nd degree 28% deep 2nd .degree 52% and su perficial 3rd degree 20% .
11. Nursing:
1. immediate treatment after hospitalization included alloting of the wards in an orderly way, establ ishing of special un rsing group, carrying out skin test. infusion. blood sample drawing. ill condition observing, intake and output volume recording. vein incision if needed and keeping adequate drainage.
2. Treating the wound surface : Debridement was done after hospitalization and MEBO was applied, The wound was kept exposed. At the early stage (in a week ) the exudate was increasing and the loss of the ointment was very quick. Application of MEBO every 3 or 5 hours was necessary. Gauze prepared by immersion in MEBO should be applied to wounds under pressure. Patients were urged to turn over regularly. For deep wounds, the smearing of the ointment should be thicker and timely clearing of the exudate was needed and necrotic tissue timely excised.
3. Nutrition+ SupplVt in addition to intravenous infusion, oral feeding of liquid diets or ordinary diets with high protein, high calorie and high vitamin was needed to ensure 3500 calorie and 100 grams of protein every day.
4. Psychofogical nursing; Help the patients todispel misgivings and to cooperate with the treatment bV doing aimed odeological work.
5. Early function training; It is helpful to the recovery of the fu notion lug of the joints.
III. Efficacy; 10 patients all healed. Patients with 3rd degree burn had scars but no contracture and the others had the extension--flexion function of their upper limbs well recovered.
IV. Experience; 1. good analgesic effect, 2. quick healing of the wound. 3. simple procedure and easy to learn, 4. no need of special facilities, 5. prevention of infections is Very important during scab dissolving period.
The Nursing of Groups of Patients with Large Area Burns Treated with MEBO
(Abstract)
Wu Yundua et al.
(People's Hospitali Xinhuang County, Hunan Province)
39 passengers were burnt when gun powder explosion happened in a train. 8 victims di.ed on the scene and 31 were hospitalized. 9 with respiratory tract burn died in a week. 12 were trasferred to other places and the remaining 10 patients were very seriously burnt. 5 had burn area more than 50% (the largest 75% )and 5 20--29% All the 10 healed by treating with MEBO.
The nursing experience is summarized as folIows:1. Strict sterilization and isolation to aviod cross infection. 2. Timely application of MEBO and cleaning of the wounds to prevent the wounds from being pressurized for a long time, thus the granulation is protected and adequate concentration of the ointment is maintained. 3. Good nutrition supply and psychological nursing.
The advantages of MEBO are : 1. No pain. 2. No infection and no deepening of the wound. 3. No scar and no need of special facilities.
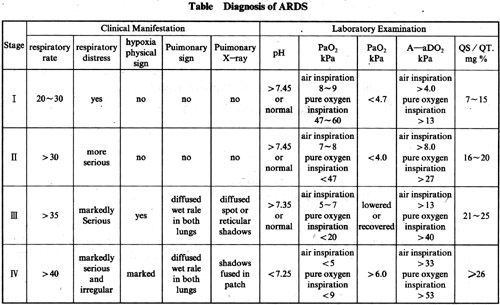
Acute Respiratory Distress Syudrome
(Abstract)
Zhang Linxiong
Since Tenken proposed for the first time in 1950. the term lung shock. acute respiratory distress syndrome has developed and many causes has been found to be responsible for ARDS. The morta--lity of this syndrome though has been reduced, it still has a death rate of 35--40%.
ARDS may be induced by shock of various causes. trauma (including major operations ), burns, inhalation of poisonous gases, disseminated intravascular coagulation, drowning, drug over--dosing, severe infections, etc.
The diagnosis of ARDS had been described in the criteria stipulated by the Three Failure Conference held in 1979. as summarized in Table.
Etiology and Mechanism :
1. Direct Causes of Lung Injury.
a. Oxygen intoxication. b. Accidental inhalation of gastric content. c.Miscellaneous. radiation injury, inhalation of poisonous gases. etc.
2. Body Fluid Factors Responsible for Lung lnjury.
Histamin, 5-HT, bradykinin. prostaglandin (including thromboxane TX A2), endotoxin. fibriongen degradation products. etc.
3. Inhibition of Reticuloendothelial System and Lack of Fibronectin.
4. Lung Injury Caused by Blood Cell Constituents. Polymorphonuclear neutrophile. blood Polymorphonuclear neutrophile. blood platelet.
5. Insufficient Lung Perfusion.
6. Lung injury Complicated with Abnormal Blood Coagulation.
disseminated intravascular coagulation over--dose of banked--blood transfusion.
7. Fat Embolism and Lipacidemia. fat embolism in diaphyses and fat embolism caused by multiple fracture.
8. Neurogenic Lung injury.
fulminant respiratory failure may occur after central nerve injury.
9. Miscellaneous.
Prevention and Treatment of ARDS:
Once ARDS occurred, the prognosis may not be good. Treatment of ARDS is a difficult and complicated task. Prevention and early treatment are very important. For patients with severe trauma and shock, the fol lowing are major points for attention :
1. Rapid restoration of blood volume after shock.
2. The patients are urged to do deep breathing.
3. Frequent change of posture,
4. Standard filter should be used for those more than 4 units of blood transfusion are needed. Obsolete banked--blood should not be used.
5. Nutrition Supply.
6. Too quick infusion should be controlled.
7: Prolonged inhalation of oxygen should be controlled.
8. Prevention of accidental inhalation of gastric content.
Two Major Links in Treating ARDS.
1. Assisted oxygen supply to maintain Sufficient oxygenation of the tissue and to support the recovery of the in injury lung.
2. Take active measure to pervent life threat--ening compl ications.
A. Oxygen Supply and Mechanical Ventilation.
For oxygen supply. catheter. rhinobyon and mask can be used at the early stage. If hypoxia can not be atleviated, mechanical ventilation is needed
1. Mechanical ventilation (see the whole text).
2. Choice of assisted breathing and externally controlled breathing. The first choice is assisted breathing. Externally controlled breathing is needed when 1, severe respiratory alkalosis. 2, severe respiratory acidosis and 3.unsynchronization of autonomous respiration and the respiration macchine.
3. Choice of Respiration Machines. It is better to choose a constant volume respiration machine.
4. Pressure Ventilation Therapy.
Intermittent assisted positive pressure respiration can be used when autonomous respiration is good. If autonomous respiration is very weak or has stopped intermittently. positive pressure ventilation is needed. If the condition is still not improved. Positive end--expiratory pressure(PEEP ) should be applied. PEEP has been proved very effective for treating ARDS. when PEEP is applied, monitoring is needed to avoid lowering of the blood pressure, decreasing of circulating blood volume. which may cause pulmonary barotrauma and pneumo--thorax.
B. External Membrane--type Oxygenator
C. Lung Transplantation
D. Artificial Lung Transplantation
E. Hypothermia Therapy
F. Controlling of Liquid Infusion and Administration of Din retics
G. Albumin Intake is a Problem of Controversy.
H. Adrenal Conical Hormone
I. Other Drugs, e.g. heparin. trasylol. isosorbide dinitrate. digitalis, respiratory stimulants and antibiotics.
J. Scopolamine is used to treat shock and to improve microcirculation and to prevent edema. Stimulation of the respiration will broaden the amplitude of respiration and alleviate the convulsions of the bronchia and reduce the secretion. It can also tranquilize the cerebral cortex and is worth of popu larization.
Recent Advances in the Treatment of Electrical injury
(Abstract)
Huang Xiaoyuan et al.
(Dept. of Burn Plastic surgery, lst Affinated Hospital, Hunan Medical university)
The number of electrical injury victims is now increasing rapidly. Disablement or even death may be caused. In this paper, the author makes are view on the recent advances in the treatment of electrical injury. Emphasizing the physiological and pathological courses and local and systemic treatments of electrical injuries and prevention of complications. A vast amount of data has been presented.
Auto--antibodies in the Serum of Burn Patients and Their Clinical Significance
(Abstract)
Liu Jiefu et al.
(Dept. of Burns,91 Hospital)
10 auto--antibodies in the serum of 360 burn patients and 120 healthy blood donors had been detected using horse redish peroxidase-- staphyIococci protein A meyhod. The results showed that in the serum of burn patients. in addition to the ordinary auto--antibodies, 3 rarely existing antibodies had been detected. namely. antilmitochondrial antibody (AMA), anti--parietal cell antibody (APCA), and anti--glomerular basement membrane antibody (AG BM). The positive rates had been 11 .1 % 5.8% and 1.7% respectively.
Clinical observations showed that the presence of AMA is interrelated with liver function injury, but has no bearing on the repeated infection of the patient. This is a consequence of autoimmuno injury of the liver after burns. The interrelation between severe anaemia at the later stage of burn and ADCA is not yet very clear. The interrelation between auto--immuno injury and AG.BM remains to be further investigated.
Statistics for Causes of Death and Anyalsis of Death Chain of Burn Patients
(Abstract)
Zhang Xiangqing, et al.
(Dept. of Burns, No. 91 Hospital)
The course of death of burn patient is very complicated. It can not be explained all sidedly .by a single cause. This paper reports an analysis of 38 cases of burn who died after receiving conventional therapy. using an expanded root death cause model. Root death cause, intermediate death cause, direct death cause bud . concomitant disease had been analyzed snd a new concept of death chain of severe burns had been introduced. This' was done in the h,ope of providing more useful information for clinical treatment and rescue of patients receiving moist therapy.
According to conventional method the 38 death cases were divided into 3 groups: children (8 cases ), adults (26 cases ) and the elderly (4 cases ). The death in children and the elderly groups had their average total burnt area and third degree burn area markedly smaller than those of the adults. This showed that death and age were Significantly interrelated. 65.8% of the death died in 10 days after burnt, this showed that at the early stage these were "many" causes which lead to death. Statistics for main complications. combined injuries and concomitant diseases revealed that the incidence of shock at early stage, hypoproteinemia. septicemia, respiratory tract burn and disturbance of water electrolyte metabolism and acid and alkali balance were higher. These complications would play a great role in the death of the patients. Analysis of causes of death revealed that though the incidence of early stage shock was a bit higher, it was not the main direct cause of death. One point that should be taken into consideration was that 4 of the patients refused to get treated. This undoubtedly accelerated the fatal complications and made the case worse. The incidence of hypoproteinemia was the highest. though it was not the direct cause of death, yet prolonged hypotonic state of the plasma colloidals was certainly responsible for the secondary abnormalities which made the case worse.
Analysis of death chain using expanded root death cause model revealed that the root death causes were the seventy of b.urn of body Surface and of respiratory tract. especially the site of the burut body su rface.
According to our data. the three main causes which were responsible for the death of most of the burn patients are namely : root death cause--severe large surface born, intermediate causeprolonged hypoproteinemia and direct cause--fatal septicemia. If there were complications of severe respiratory tract burn, the death chain would certainly become more complicated. A discussion has been presented.